

 Management of the masseter muscle is one of the key technical issues in placement of isolated jaw angle and wraparound jawline implants. This applies to all implant sized and dimensions but particularly vertical-lengthening or large widening angle implants. It is also pertinent to any jaw angle that has had prior surgery, such as SSROs and V line surgeries, prior to implant placements.
Management of the masseter muscle is one of the key technical issues in placement of isolated jaw angle and wraparound jawline implants. This applies to all implant sized and dimensions but particularly vertical-lengthening or large widening angle implants. It is also pertinent to any jaw angle that has had prior surgery, such as SSROs and V line surgeries, prior to implant placements.
Surgical Approaches
1. Subperiosteal Dissection Deep to the Masseter
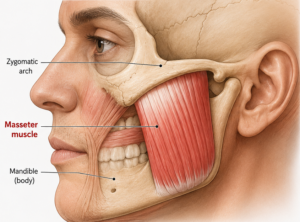
All custom and standard angle implants are placed in a subperiosteal pocket on the lateral mandibular ramus and angle, which requires elevation of the masseter muscle from the bone and along its insertion points over the angle.
Key points:
- The masseter is detached only as much as necessary to create the implant pocket.
- The periosteum and masseter are elevated together as a composite layer.
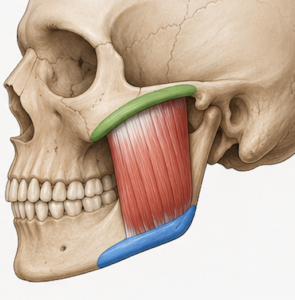
- It is the ligamentous attachments along the inferior bony border that are the critical areas of release (blue zone) Aggressive stripping of these ligaments off of the bone is why masseter msucle dehiscence and retraction occurs.
Reattachment and Healing
After implant placement:
- The masseter is not and can not be formally sutured back to the mandible.
- The muscle reattaches spontaneously to the implant-covered mandibular surface through scar tissue and soft tissue adaptation.
- Stable fixation of the implant with screws is essential because muscle forces are substantial.
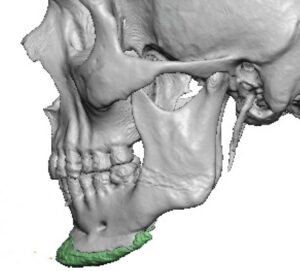
Vertical-Lengthening Jaw Angle Implants
This situation presents unique considerations.
When the implant extends the angle inferiorly:
- The implant creates a new lower mandibular border beneath the original muscle insertion.
- The muscle will only follow the implant downward (lengthen) if its periosteal sling attachments remain intact and there are limits as how much it will do so.
- The ligamentous insertion must be released but the wrap around periosteum must remain intact.
- The larger the vertical implant drop the greater the risk of the muscle not following the implant downward (masseteric muscle dehiscence)
As a result:
- The risk is that the lower portion of the implant is only covered by soft tissue rather than masseter muscle.
- If it occurs it is an aesthetic soft contour deformity with no functional significance.
- In thin patients the implant may be very visible (skeletonized) with almost only skin over it. (implant reveal)
Muscle-Related Postoperative Issues
Early Trismus
Common for 2–6 weeks due to:
- Masseter elevation
- Muscle edema
- Reflex spasm
Management:
- Jaw-opening exercises
- Soft diet initially
- NSAIDs/steroids when appropriate
Chronic Tightness
Occasionally patients experience:
- Persistent masseter tightness
- Difficulty with maximal opening
Usually improves over several months as the muscle adapts to the new skeletal contour.
Implant Mobility
If fixation is inadequate:
- Repetitive masseter contraction can produce micromotion.
- This may lead to pain, fibrous encapsulation, or malposition.
Rigid screw fixation largely prevents this problem.
Custom Jaw Angle Implants
With modern custom implants:
- The design should account for the masseter footprint.
- Excessive lateral projection directly beneath the thickest portion of the muscle can increase soft-tissue tension and palpability.
- Smooth transitions along the ramus help the muscle drape naturally over the implant.
Practical Surgical Principle
The masseter muscles ligamentous attachments should be elevated with care to prevent insertion detachment and retraction. Should the muscular sling attachments be seen to be detached intraoperatively, which is often not obvious intraorally, attempts to reattach the muscle are usually not successful. There are suture bolster techniques that can be tried but the implant works against success.
For very large custom angle implants (especially >10–12 mm vertical lengthening), the relationship between the original masseter insertion and the new inferior border becomes an important design consideration and potential implant-muscle mismatch.
Preoperative consideration of the masseter muscle in jaw angle implant surgery
The main considerations are:
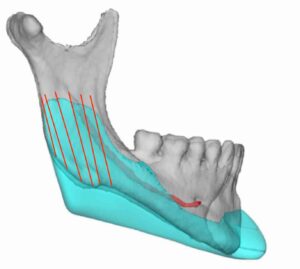
- Assess the risk of masseteric muscle dehiscence by the bony angle anatomy seen on the 3D CT scan
- Evidence of bony prominences/spikes indicate strong masseter muscle ligamentous attachments whose releases are more difficult with a higher risk of masseteric muscle dehiscence
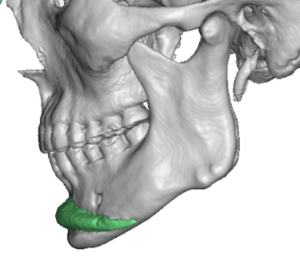
- Prominent antegonial notch with high jaw angle indicates strong muscle pull and short masseter muscle length
- Consider lesser amounts of vertical implant lengthening in high risk patients
- Consider preoperative Botox in selected cases of significant masseter hypertrophy associated with symptomatic clenchung/bruxism
Dr. Barry Eppley
Plastic Surgeon