

Prominent lower ribs that project outward beneath the breast crease or upper abdominal area, can be treated by rib shaving (rib contouring) to reduce their flared appearance.
When rib shaving may help
Rib contouring is most effective when:
- The lower costal margin (typically ribs 8–10) is excessively prominent.
- The flare is due to actual rib projection rather than posture, muscle imbalance, or scoliosis.
- The patient has a thin body habitus where the rib prominence is visible despite low body fat.
The procedure generally involves:

- Limited resection or contouring of the most prominent portion of the costal cartilage and/or rib.
- Small incisions placed in the upper abdominal area dierctly over the prominences.
- Preservation of chest wall stability and protection of underlying structures.
When rib shaving may not help
If the flare is caused by:
- Anterior pelvic tilt or postural issues.
- Pectus deformities.
- Scoliosis or rotational chest wall asymmetry.
- Abdominal muscle weakness.
Then surgery on the ribs alone may provide little improvement.
Alternatives
Depending on the anatomy:
- Costal cartilage reshaping by higher levels of osteotomies and plate fixation.
- Fat grafting around adjacent areas to camouflage the prominence.
- Physical therapy when posture contributes significantly.
Evaluation
For surgical planning, I typically recommend:a CT scan of the chest/upper abdomen with 3D reconstruction if the anatomy is unusual or significant asymmetry exists.
The key question is whether the flare is:
- Bilateral and symmetric, producing a broad lower ch
- est appearance, or
- Unilateral/asymmetric, where one side projects more than the other.
Case Example

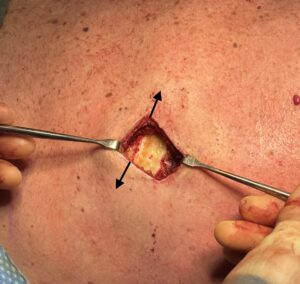
 This male was having pectoral implant replacements and asked about reduction of his subcostal flaring. He had a flared lower ribcage and well developed rectus abdominal muscles. Give his well developed body and exercise regimen osteotomies and corseting was not seen as a viable option. It also was not his highest body contouring priority. From an open excision approach I did not want to cut through his rectus muscle (outline of the rectus abdominus muscle seen in yellow) so a lateral approach was planned, reaching up under the muscle from the side and getting as much prominence reduction as that access would allow. But with the understanding much of the prominence behind the rectus muscle would not be reduced in the main effects of the shaving would be lateral to the muscle.
This male was having pectoral implant replacements and asked about reduction of his subcostal flaring. He had a flared lower ribcage and well developed rectus abdominal muscles. Give his well developed body and exercise regimen osteotomies and corseting was not seen as a viable option. It also was not his highest body contouring priority. From an open excision approach I did not want to cut through his rectus muscle (outline of the rectus abdominus muscle seen in yellow) so a lateral approach was planned, reaching up under the muscle from the side and getting as much prominence reduction as that access would allow. But with the understanding much of the prominence behind the rectus muscle would not be reduced in the main effects of the shaving would be lateral to the muscle.
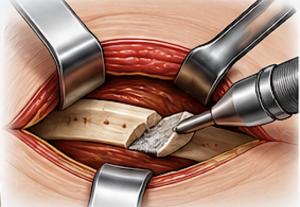
 Under general anesthesia lateral subcostal incisions were marked and used for access. The subcostal rib shaving was done after the completion of pectoral and bicep implants. Using a high-speed hand piece and burr the outer layer of the rib prominence was reduced leaving a thinner inner layer. The reduction was carried as far forward and behind the incision along the length of the rib as possible based on the stretch of the skin.
Under general anesthesia lateral subcostal incisions were marked and used for access. The subcostal rib shaving was done after the completion of pectoral and bicep implants. Using a high-speed hand piece and burr the outer layer of the rib prominence was reduced leaving a thinner inner layer. The reduction was carried as far forward and behind the incision along the length of the rib as possible based on the stretch of the skin.

 The immediate effects of the reduction could be seen along the lateral subcostal prominence as was preoperatively expected. Int other words some minor improvements but certainly not anoverall reduction in the subcostal rib flare in its entirety.
The immediate effects of the reduction could be seen along the lateral subcostal prominence as was preoperatively expected. Int other words some minor improvements but certainly not anoverall reduction in the subcostal rib flare in its entirety.
Discussion
Like all rib removal/contouring surgeries the initial question is always one of safety. In properly selected patients, subcostal rib shaving/contouring can be performed safely, but it is important to recognize that the lower ribs lie directly over the pleura, diaphragm and upper abdominal organs.
Main safety considerations
1. Chest wall stability
The greatest concern is removing too much rib or cartilage.
- Limited contouring of the most prominent edge is generally well tolerated.
- Aggressive resection can weaken structural support and potentially create contour irregularities or chronic discomfort.
- By definition rib shaving is not the same as rib removal and it preserves the inner layer of the rib(s) and only reduces the outer protruding portion.
2. Pleural injury
The pleural lining of the lung lies immediately deep to the ribs.
- A tear can cause a pneumothorax (collapsed lung).
- While uncommon in experienced hands, it is a recognized risk (I have yet to see it)
- If it occurs, temporary chest drainage may be required. (rare)
3. Chronic pain or sensory changes
Intercostal nerves run along the underside of each rib.
- Temporary numbness is common.
- Persistent numbness or neuralgia is uncommon but possible.
- Excessive reduction increases the risk.
5. Cosmetic irregularities
Potential aesthetic issues include:
- Undercorrection
- Residual asymmetry
- Overresection causing depressions
- Visible contour transitions
Who is the best candidate?
The safest and most predictable candidates are:
- Thin or athletic patients
- True bony/cartilaginous rib prominence
- Symmetric subcostal flaring
- Realistic expectations regarding the amount of rib prominence reduction possible
My view on safety
For modest subcostal flare correction, limited contouring of ribs 8–10 or their costal cartilages can usually be done with an acceptable safety profile. The risks increase as more rib is removed or when multiple ribs are extensively resected solely for rib prominence reduction.
A preoperative CT scan with 3D reconstruction is often useful because it shows exactly which ribs are involved and the location of their greatest prominence.
Dr. Barry Eppley
Plastic Surgeon