

The deep plane facelift is based on a detailed understanding of the layered anatomy of the face and the relationship between the skin, SMAS (superficial musculoaponeurotic system), facial mimetic muscles, retaining ligaments, and facial nerve branches.
Fundamental Anatomical Concept
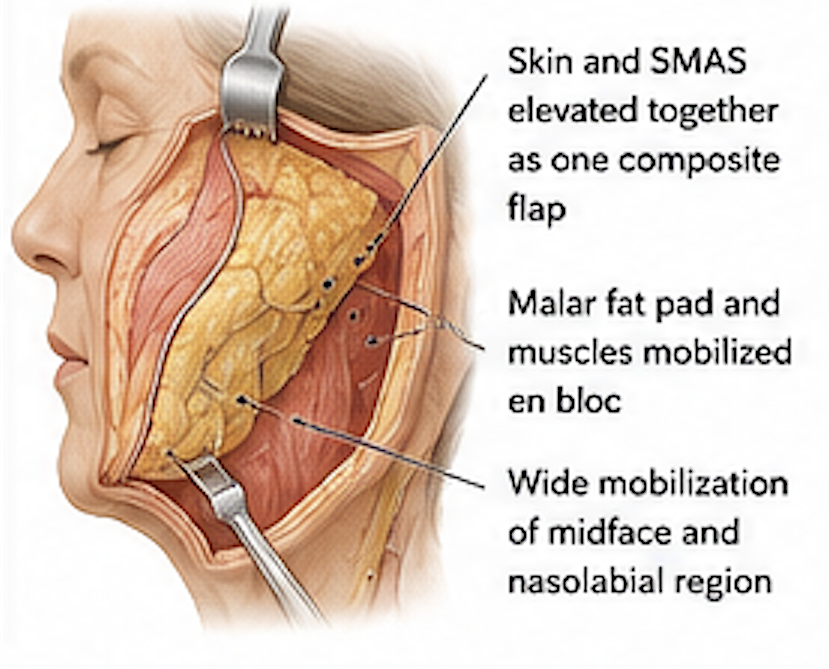
Traditional SMAS facelifts elevate the skin and SMAS as separate layers or manipulate the SMAS superficially. In contrast, a deep plane facelift elevates the skin and SMAS together as a composite flap, entering the plane deep to the SMAS in the midface.
The rationale is that the major age-related descent of the cheek occurs in structures that are anatomically bound together:
- Skin
- SMAS
- Platysma
- Zygomaticus major and minor muscles
- Malar fat pad
These structures form a functional unit that descends with aging.
Key Anatomical Structures
1. The SMAS
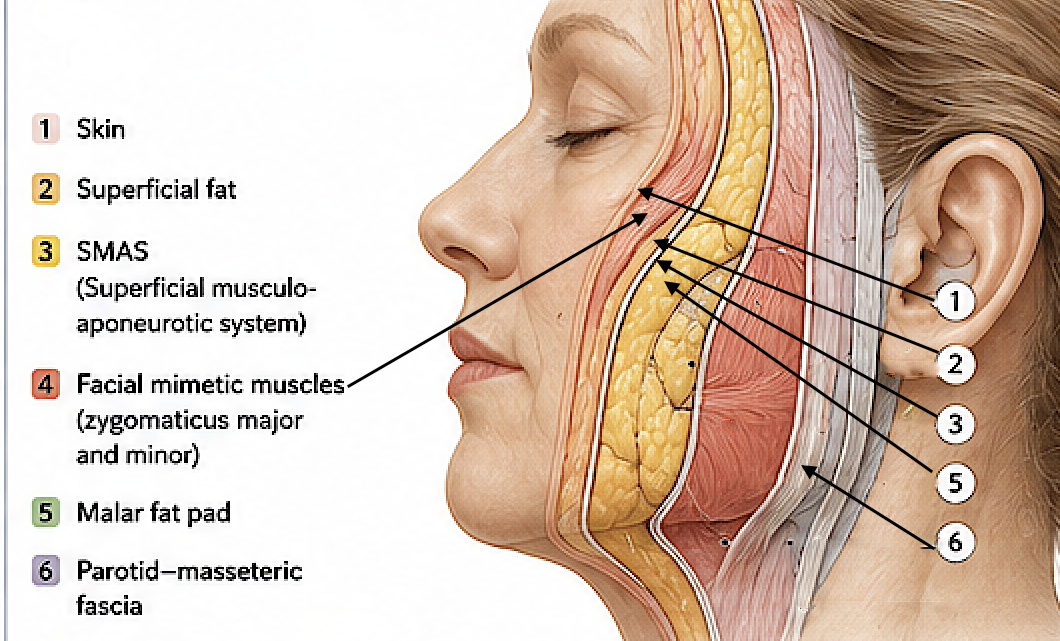
The SMAS is a fibromuscular layer extending from:
- Platysma in the neck
- Parotid fascia in the cheek
- Temporoparietal fascia superiorly
The SMAS envelops and transmits force to the muscles of facial expression.
The deep plane facelift recognizes that the malar fat pad is attached to the SMAS-muscular complex, and therefore lifting only the skin or superficial SMAS often fails to restore youthful midface volume.
2. Retaining Ligaments
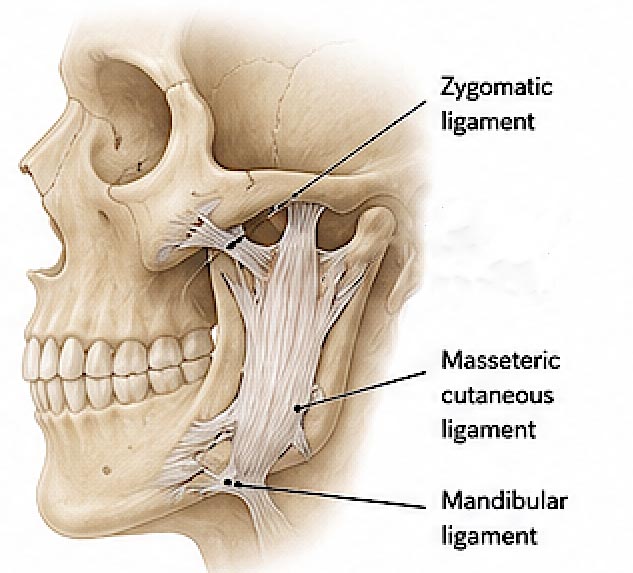
The retaining ligaments are the principal anatomical basis for the operation.
Important ligaments include:
Zygomatic Ligaments
- Attach periosteum of the zygoma to the dermis.
- Strongly tether the cheek.
Masseteric Cutaneous Ligaments
- Connect the masseteric fascia to skin.
- Create fixation points in the lower face.
Mandibular Ligaments
- Contribute to jowl formation.
Aging causes soft tissues to descend around these fixed points.
The deep plane facelift works by:
- Releasing these retaining ligaments
- Mobilizing the composite SMAS-cheek flap
- Allowing vertical repositioning of descended tissues
Without ligament release, only limited movement is possible.
3. The Prezygomatic Space
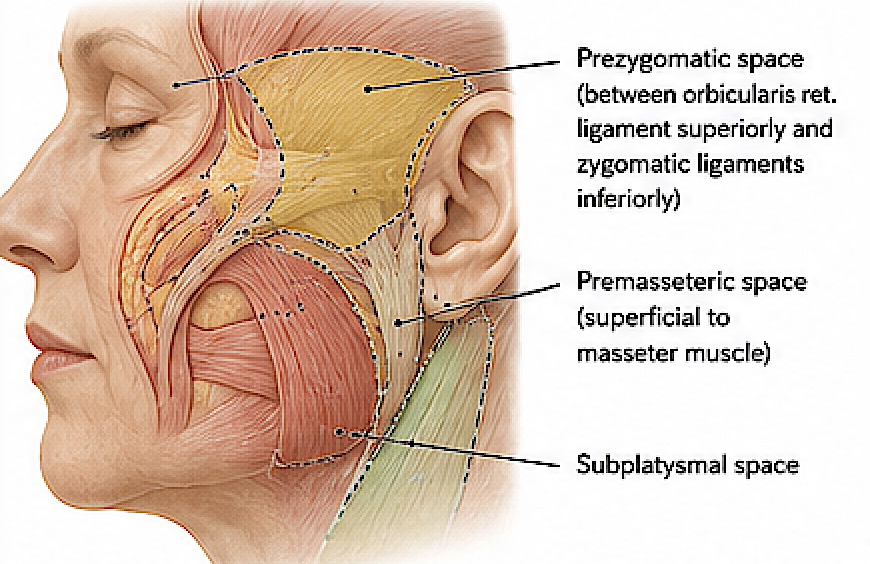
This is one of the most important anatomical spaces in deep plane surgery.
Boundaries:
- Superior: orbicularis retaining ligament
- Inferior: zygomatic ligaments
- Deep: periosteum and deep fascia
- Superficial: orbicularis oculi and SMAS
This space provides a relatively safe plane for mobilizing the midface while avoiding facial nerve injury.
4. Facial Nerve Anatomy
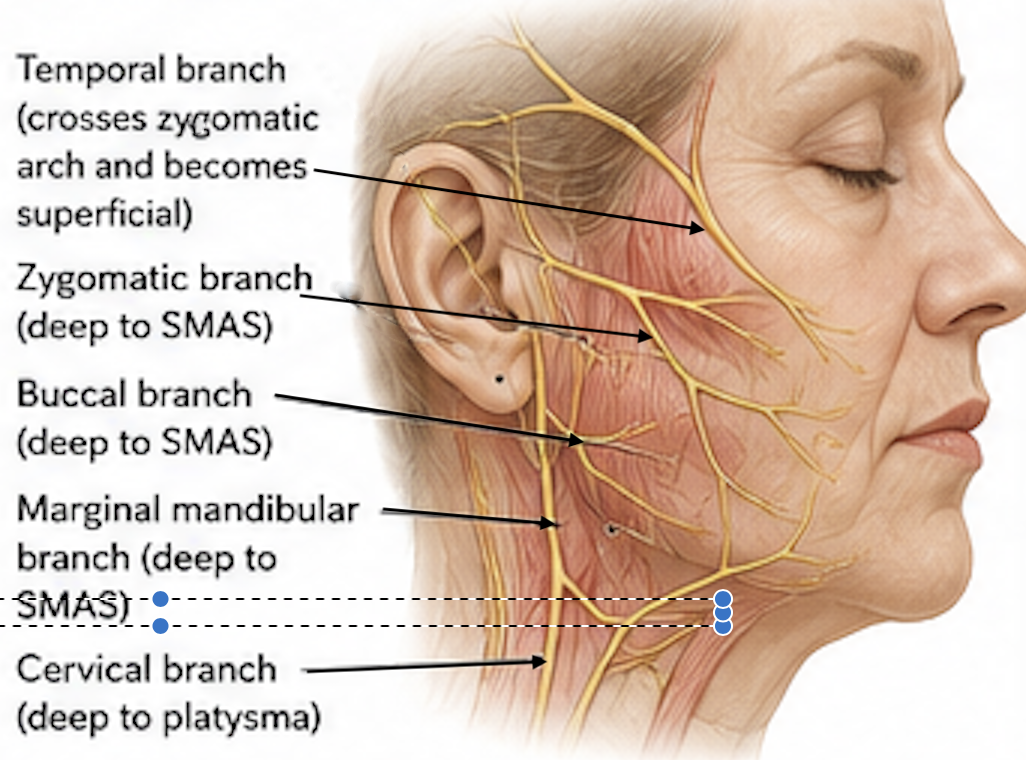
The facial nerve branches lie deep to the SMAS in most of the cheek.
Important relationships:
Temporal Branch
- Vulnerable near the zygomatic arch.
- Crosses from deep to superficial.
Zygomatic and Buccal Branches
- Generally remain protected deep to the dissection plane.
The deep plane facelift takes advantage of this anatomy because:
- The dissection proceeds in natural areolar planes.
- Most facial nerve branches remain on the deep surface.
This permits extensive mobilization with relatively low nerve injury risk when performed correctly.
Midface Rejuvenation
One of the principal anatomical advantages of the deep plane technique is direct mobilization of:
- Malar fat pad
- Nasolabial complex
- Orbicularis oculi-cheek unit
This produces:
- Elevation of the cheek
- Softening of the nasolabial fold
- Improvement of the lid-cheek junction
- Reduction of jowling
These changes are more difficult to achieve with traditional lateral-vector SMAS tightening alone.
Aging Changes Addressed by the Deep Plane
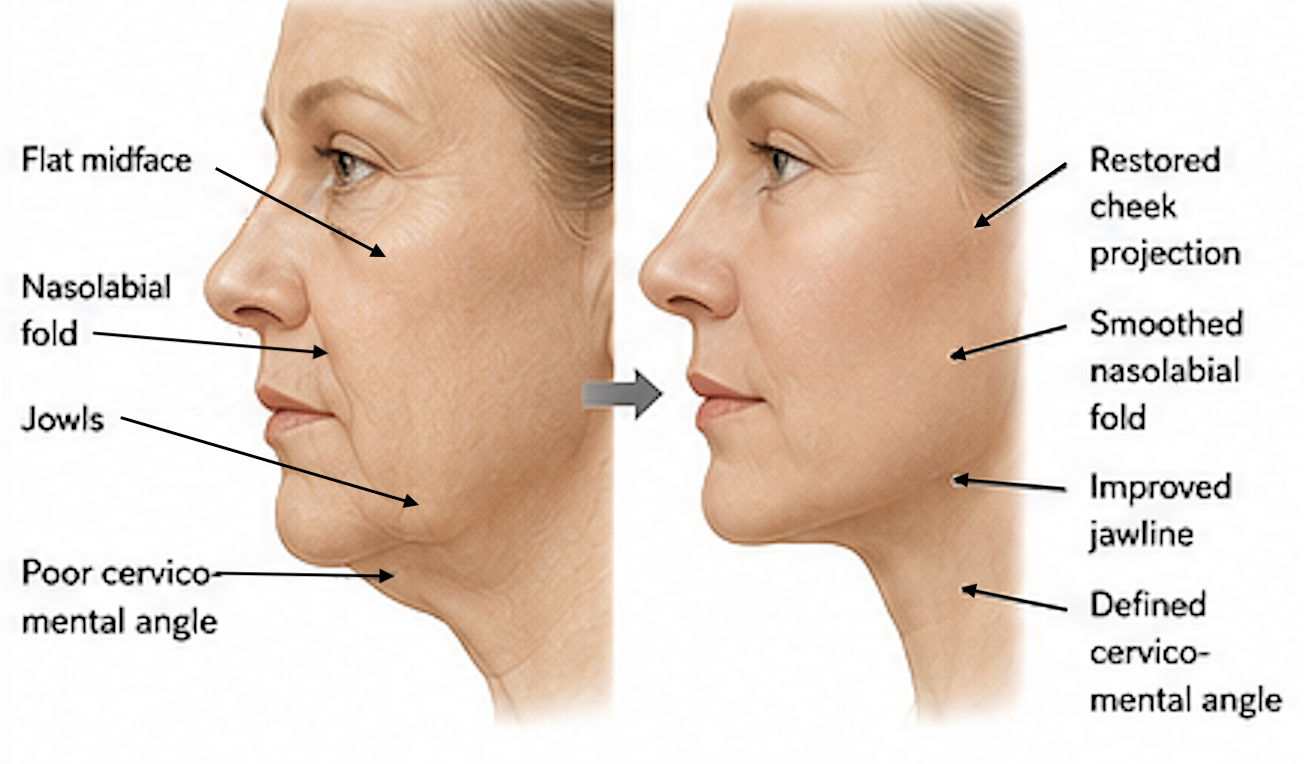
Aging produces:
- Ligamentous attenuation
- Descent of the malar fat pad
- Volume redistribution
- Jowl formation
- Deepening of the nasolabial fold
The deep plane facelift restores anatomy by:
- Releasing retaining ligaments
- Repositioning descended soft tissues as a single unit
- Restoring the cheek mass superiorly and posteriorly
Modern Anatomical Understanding
The contemporary deep plane facelift is heavily influenced by recent anatomical work with the concept of facial spaces and retaining ligaments providing the strongest anatomical justification for deep plane surgery, demonstrating that facial aging is largely a problem of soft-tissue descent constrained by ligamentous fixation rather than simply skin laxity.
In summary
The anatomical basis of the deep plane facelift is the recognition that facial aging results from descent of the integrated SMAS-muscle-malar fat pad complex around fixed retaining ligaments. By dissecting beneath the SMAS, releasing the zygomatic and masseteric retaining ligaments, and mobilizing the composite cheek flap through the prezygomatic and premasseter spaces, the surgeon can reposition the midface and lower face in a more anatomical and durable manner than skin-only or superficial SMAS techniques.
Dr. Barry Eppley
Plastic Surgeon