

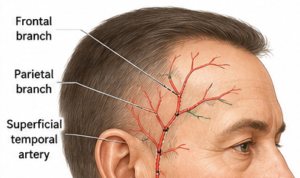

The superficial temporal artery is prone to become visibly prominent for a variety of reasons particularly in man. A prominent temporal artery is most commonly a cosmetic concern although it is possible that it may also be a sign of temporal migraines and other medical conditions. While the temporal artery is frequently shown in anatomic illustrations as a relatively straight arterial course it is well-known that it has an extremely serpiginous appearance as it crosses into the forehead.


For cosmetic reduction of prominent temporal arteries, the success rate is generally very high when the artery is properly mapped and ligated at all inflow and outflow points. This always starts as three basic ligation points (most proximal, most distal and midway between the two). But in the actua ligation procedure the number of ligation points is increased until there is no l0nger any audible signal in it by doppler ultrasound. A s a result most patients end up with four (4) ligation areas per side.
 While the procedure ends with no audible signal along the preop course of the artery what is the long term success in terms of prominence reduction or elimination? The best available published and clinical data suggest:
While the procedure ends with no audible signal along the preop course of the artery what is the long term success in terms of prominence reduction or elimination? The best available published and clinical data suggest:
- ~85–90% of patients achieve a satisfactory result after a single procedure. In my experience 86% required only one procedure, while about 13% underwent a second procedure because of persistent collateral flow with partial recurrence of a portion of the artery.
- When secondary touch-up ligation was performed, the reported patients did not require further surgery.
- Recurrence appears uncommon and is usually due to missed collateral branches rather than true regrowth of the artery.
- In my experience prominent temporal arteries can be substantially reduced or completely eliminated, but long-term success depends on identifying both antegrade and retrograde blood flow pathways.
In practical terms, for a patient with a classic visible, pulsatile superficial temporal artery, I would generally quote:
- 80–90% chance of a very good cosmetic improvement
- 50–80% chance of complete disappearance, depending on anatomy and collateral circulation
- 10–20% chance of needing a minor secondary ligation procedure for residual filling from collateral branches
The biggest determinant of success is not the ligation itself but accurately identifying all feeding branches preoperatively (often with Doppler ultrasound) and performing multilevel ligation rather than a single tie-off.
Dr. Barry Eppley
Plastic Surgeon