

The surgical placement of aesthetic hip implants is dictated by the soft tissue anatomy between the iliac crest and the greater trochanter of the femur. While it would be ideal to place the implant in a subfascial or submuscular plane over the lateral pelvis where the implant is protected and edges would have no risk of being seen the anatomy of the lateral pelvis makes this impractical in most cases.
Lateral Pelvic Anatomy
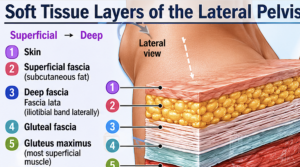
The soft tissue layers of the lateral pelvis (lateral hip/gluteal region) can be described from superficial to deep as follows:
- Skin
- Superficial fascia (subcutaneous tissue)
- Variable thickness of adipose tissue
- Contains superficial nerves and vessels
- Deep fascia
-
- Fascia lata over the lateral thigh
- Thickening of the fascia lata forms the iliotibial band (IT band) laterally
- Continuous superiorly with gluteal fascia
- Gluteal fascia
-
- Covers the gluteus medius and gluteus maximus
- Attaches to the iliac crest and blends with fascia lata
- Gluteus maximus muscle (posterolateral pelvis)
-
- Most superficial gluteal muscle
- Fibers insert into the IT band and gluteal tuberosity
For the Hip Dip Region Specifically

The typical sequence from superficial to deep is:
- Skin
- Subcutaneous fat
- Superficial adipose layer
- Fibrous septae
- Superficial fascial system (SFS)
- Deep subcutaneous fat
- Deep fascia
-
- Gluteal fascia superiorly
- Fascia lata laterally
The major structure of concern potentially encountered in this region is the:
Lateral femoral cutaneous nerve (LFCN)
- Passes near the ASIS
- Travels beneath or through the inguinal ligament
- Supplies sensation to the lateral thigh
Injury can cause:
- Meralgia paresthetica
- Burning pain
- Numbness of lateral thigh
The nerve lies:
- Anterior to the typical hip dip augmentation zone so the risk of injury is low
- Closest to risk near the ASIS
Common Pocket Locations
1. Deep Subcutaneous Placement (on top of TFL fascia)
Most common for moderate to large-sized implants.
Advantages:
- Simpler dissection
- Less postoperative pain
- Preserves muscle function
- Good implant control
- Disadvantages:
- Less soft-tissue coverage
- Greater risk of edge visibility in thin patients
2. Subfascial Placement
Typically beneath the tensor fascia lata fascia and on top of muscle.
Advantages:
- Better implant camouflage
- Less palpability
Disadvantages:
- Only small implants can be placed
- Greater postoperative discomfort
- Limited aesthetic augmentation
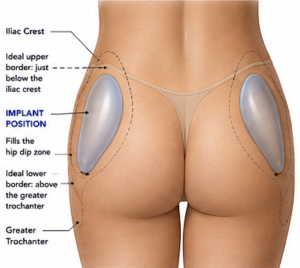
The implant pocket should:
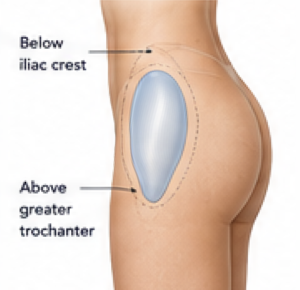
Begin just below the iliac crest
End around the greater trochanter
Fill the hip-dip zone
Remain centered over the lateral pelvis
Avoid extending excessively into the buttock
Avoid crossing too far anteriorly onto the anterior thigh
Incision Options
Superior Iliac Crest Incision
Most common.

5-7 cm incision
Advantages:
- Hidden in underwear
- Direct access to pocket
- Easer to achieve bilateral symmetry
Lateral Buttock Incision

Used when combined with gluteal augmentation.
Advantages:
- Single operative field
Disadvantages:
- Longer dissection tunnel
- More difficult pocket control
Pocket Design Principles
The pocket should be:
- Slightly larger than implant dimensions
- Tight enough to prevent migration
- Symmetrical bilaterally
- Created to match the custom implant geometry
A common cause of malposition is a pocket that is wider and longer than the implant.
Fixation
Many custom silicone hip implants are placed without fixation because:
- The pocket provides control
- Broad implant surface area resists rotation
Fixation methods available:
- ePTFE strips on underside of implant
- Perfusion holes
- Iliac crest suture suspension
The implant shape and the pocket should be designed together. A technically perfect implant can fail aesthetically if the pocket does not match its geometry. For custom implants, the surgical plane often influences the final implant thickness and edge taper as much as the desired external contour.
Dr Barry Eppley
Plastic Surgeon