


 Superficial temporal artery prominence is well known to occur and for some affected fond it to be an aesthetic concern. The definitive treatment is to reduce/eliminate the flow through the visible part of the artery by a ligation technique. Due to the extensive connections or anastomoses of the artery, as is common for many head and neck vessels, shutting off the flow through the artery is not as simple as it may seem as it is not a ‘straight line single pipe.’
Superficial temporal artery prominence is well known to occur and for some affected fond it to be an aesthetic concern. The definitive treatment is to reduce/eliminate the flow through the visible part of the artery by a ligation technique. Due to the extensive connections or anastomoses of the artery, as is common for many head and neck vessels, shutting off the flow through the artery is not as simple as it may seem as it is not a ‘straight line single pipe.’
As a result ligation of the superficial temporal artery requires multiple sites, most of which are visible but some are not. How many such ligation sites that are needed will vary per patient with the end goal of eliminating the blood flow through the visible section of the artery.
Case Study
This middle-aged male developed prominent temporal arteries once he lost weight and starting exercising regularly including boxing. When presenting for ligations, as is common, the artery’s prominence and tortuosity is less apparent.
 But careful inspection and palpation allows the arterial course to be charted and key ligation sites marked. How many ligation sites are marked depends on its branch sites distal to the primary proximal ligation site which is usually at least two.
But careful inspection and palpation allows the arterial course to be charted and key ligation sites marked. How many ligation sites are marked depends on its branch sites distal to the primary proximal ligation site which is usually at least two.

 Under local anesthesia the three primary ligation sites wer opened with a small incision. The artery was identified and a loop of the artery pulled out of the incision after dissection where double 5-0 ties are placed. The loop is dropped back in and the incision closed with small 6-0 plain sutures,
Under local anesthesia the three primary ligation sites wer opened with a small incision. The artery was identified and a loop of the artery pulled out of the incision after dissection where double 5-0 ties are placed. The loop is dropped back in and the incision closed with small 6-0 plain sutures,
 After the three primary sites wee ligated a dopper check showed residual signals which required two additional ligation sites for a total of five small incisions.
After the three primary sites wee ligated a dopper check showed residual signals which required two additional ligation sites for a total of five small incisions.
Discussion
The number of ligation sites needed in a superficial temporal artery (STA) ligation depends on the indication for surgery. For aesthetic treatment of prominent, enlarged, pulsatile temporal arteries, a single ligation is always insufficient because of the extensive collateral circulation of the scalp.
Typical Number of Ligation Sites
- 1 ligation site
- Never adequate/works except for a very focal arterial prominence.
- High likelihood that the artery will continue to fill retrograde from collateral vessels.
- 2 ligation sites
- One proximal and one distal to the visible segment.
- Theoretically this should work but never does again due to the extensive collateral blood flow
- 3–5 ligation sites
- This is the normal number of ligation sites needed for serpiginous arteries.
- Additional ligations are placed where collateral inflow is identified.
- Common in patients with bilateral, highly tortuous arteries extending across much of the temple and forehead.
- More than 5 sites
- Occasionally necessary in patients with diffuse enlargement involving multiple branches.
- This is uncommon but not unusual in patients with longstanding vascular prominence with a large number of branches
Why Multiple Ligations Are Often Necessary
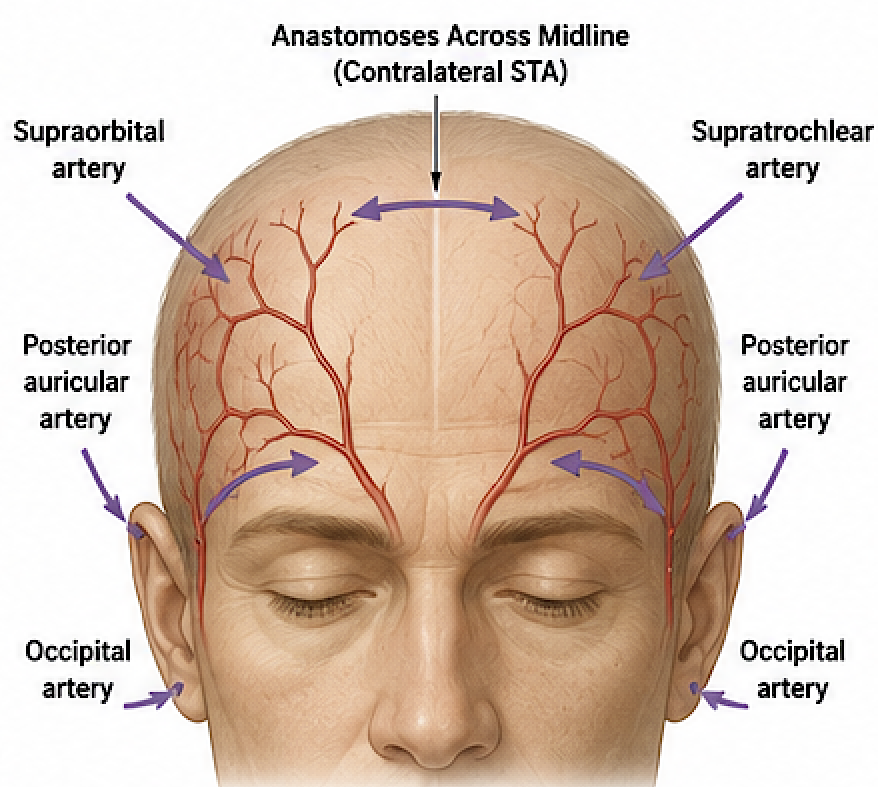
The superficial temporal artery has extensive anastomoses with:
- Contralateral superficial temporal artery
- Supraorbital artery
- Supratrochlear artery
- Occipital artery
- Posterior auricular artery
Because of these collateral pathways, simply tying off one point allows the vessel to refill from the opposite direction.
Role of Doppler Ultrasound
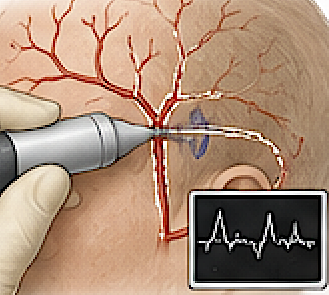
A handheld Doppler has become one of the most valuable adjuncts during surgery because it allows:
- Mapping the entire arterial course before incisions.
- Identify dominant inflow branches.
- Confirm cessation of flow after each ligation.
- Detect persistent retrograde flow requiring additional ligation.
- Reduce unnecessary incisions while minimizing recurrence.
In my view, Doppler-guided temporal artery ligation is considerably more reliable than relying on visual inspection or palpation alone.
Practical Surgical Experience
For cosmetic temporal artery ligation, I find that the average case requires 3 to 5 ligation sites. Three incisional sites are preoperatively marked and then opened and ligated. Then a Doppler check is done from which additional ligations are done based on the detection of residual pulsatile signals.
Key Principle
The objective is elimination of blood flow through the visible arterial segment. Ligations are not completed until a Doppler confirms there is no residual flow along the cosmetically visible portion of the artery..
Barry Eppley, MD, DMD
Plastic Surgeon