

In rib removal surgery of the lower rib cage for a waistline narrowing effect the most feared complication is that of a pneumothorax. A pneumothorax occurs because the pleural lining of the lung is inadvertently opened or torn during surgery and is not recognized. This allows air to escape from the lungs and, if enough air does escape, the affected lung side can partially collapse, creating some level of respiratory insufficiency postoperatively. In the worst case scenario this results in the need for a chest tube for re-inflation of the lung.
The pertinent question is how often does a pneumothorax occur and how does it compare to pleural visibility.
The short answer is I have yet to have an actual pneumothorax in over 500 ribs removed. However, visualizing the pleura in some cases at certain rib levels is not completely rare.
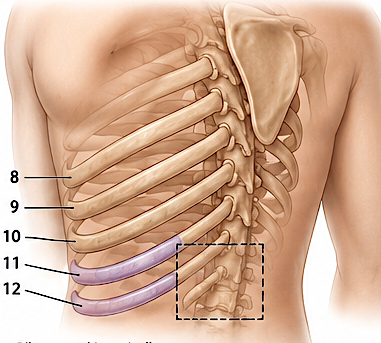
In my experience with aesthetic rib removal surgery (10, 11th and 12th ribs), the parietal pleura is visualized in perhaps 3% to 5% of cases, depending on the patient’s anatomy and the extent of periosteal dissection. Seeing the pleura is not the same as violating it.
Why the pleura becomes visible
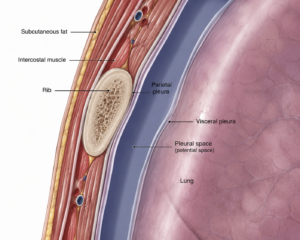
The posterior portions of the lower ribs have a very thin layer of endothoracic fascia separating the rib from the parietal pleura. During subperiosteal dissection:
- The periosteum is elevated from the rib.
- Near the rib neck and posterior third of the rib, the tissue becomes increasingly thin.
- The glistening white-blue parietal pleura may become visible through the endothoracic fascia.
This is particularly common in:
- Thin patients (BMI <22)
- Females with little retroperitoneal fat
- Patients undergoing maximal posterior rib removal
- The 10th rib, which lies closer to the pleural reflection than the floating ribs
Seeing versus entering the pleura
There is an important distinction.
Pleura visualized

- Smooth, shiny membrane
- No air leak
- Lung may be seen moving up and down with inspiration
- No pneumothorax
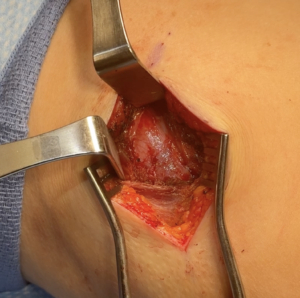
intact pleura with lung movement DrfBarry EppleyThe pleura is very thin and easy to violate without good surgical technique particularly at rib number 10, where it is likely to be found on the backside of the removed rib. This can be seen in the attached video where the parietal pleura is intact and the lung can be seen moving up and down with inspiration.
Pleura entered
- Small tear in membrane
- May have audible air movement or bubbling
- Visible lung movement beneath the opening
- Potential risk of postoperative pneumothorax
Estimated incidence
Of the plural visibility that I have seen only a very small percent have been actual pleural tears (less than 10). These pleural openings are small and are repaired immediately with muscle grafts (taken from the nearby latissimus dorsi muscle) sewn over themwith intraoperative lung inflation confirming a good seal.
Surgical pearls
The safest dissection remains:
- Strictly subperiosteal
- Keep the elevator on bone at all times
- Avoid blind posterior sweeping motions
- If a pleural tear is seen remove enough rib around it so that it can be adequately repaired
Bottom line
Visualization of the parietal pleura during lower rib removal is not unusual and should not be considered a complication. It simply reflects the close anatomical relationship between the posterior lower ribs and the thoracic cavity. The key distinction is that seeing the pleura requires no treatment, but entering it does. Immediate repair avoids the risk of postoperative pneumothorax.
Dr. Barry Eppley
Plastic Surgeon