


The.most common facial defatting procedure, a buccal lipectomy, is seemingly a straight forward and effective procedure. But like all aesthetic surgeries there are downsides and errors with it.
Common buccal lipectomy (buccal fat removal) errors can be divided into planning errors and technical surgical errors.
Patient Selection Errors
These are often the most significant misjudgements.

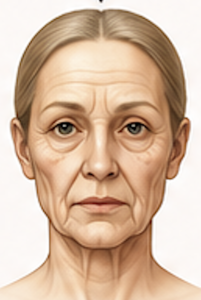
- Performing the procedure on naturally thin-faced patients
- Can create a prematurely aged appearance.
- Midface hollowing may become progressively more apparent with age.
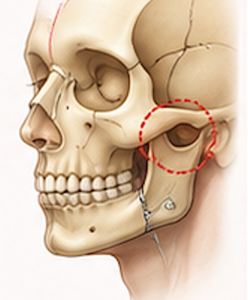
- Ignoring facial skeletal anatomy

- Patients with weak malar projection or maxillary deficiency often benefit from cheekbone augmentation rather than volume reduction.
- Overestimating the contribution of buccal fat
- Many “full” faces are due to subcutaneous fat, masseter hypertrophy, or skeletal structure rather than buccal fat alone.
- It is common that the exact anatomic affects of a buccal lipectomy are not understood and its effects are much more inferior then what they are.
- Some patients would benefit better with periorak/lateral facial micro-liposuction either alone or as a complement to subtotal buccal lipectomies for achieve their desired effects.
- Failure to assess aging trajectory
- Young patients may look excellent initially but develop excessive hollowing 10–20 years later.

Surgical Technique Errors
Excessive Fat Removal
The most common technical error.
- Overresection can produce:
- Hollow cheeks
- Skeletonized appearance
- Premature aging
- Visible depression beneath the zygoma
Because the buccal fat pad is difficult to replace predictably, overresection is a major concern. Some patients may only need a subtotal buccal lipectomy,
Asymmetric Fat Removal
- Unequal extraction between sides.
- Results in facial asymmetry that may be difficult to correct.
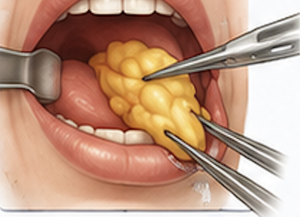
Failure to Remove The Actual Buccal Fat Pad
The buccal fat lies deeper than some realize and it has a very distinct appearance from other facial fat. Also there is a small fat collection more superficial right under the mucosa.
Errors include:
- Removing the smaller superficial fat instead (not going deep enough)
- This should not be confused with a subtotal buccal lipectomy
Consequences:
- No external reduction effect
Facial Nerve Injury

The buccal branches of the facial nerve are nearby.
Possible errors:
- Dissection outside the proper plane.
- Excessive cautery.
- Aggressive traction.
Consequences:
- Weakness of upper lip movement.
- Smile asymmetry.
- Usually temporary, occasionally prolonged.
Parotid Duct Injury
The Stensen duct lies close to the surgical field.
Technical errors include:
- Incorrect incision placement.
- Catching the duct with sutures in the mucosal closure
Potential outcomes:
- Salivary outflow obstruction
- Duct stenosis
- Need for secondary repair
Hemostasis Errors
The buccal fat pad has a main arterial supply at its base which is why it is used in reconstruction of intraoral regional defects.
Technical errors include:
- Failure to identify vascular pedicle and cauterize it
- Aggressive avulsion
Can lead to:
- Hematoma
- Swelling
- Increased infection risk
- Delayed recovery
Closure Errors
- Inadequate mucosal closure.
- Excessive tension.
- Poor tissue handling.
May result in:
- Wound breakdown
- Delayed healing
- Oral contamination
Long-Term Adverse Aesthetic Outcomes

These are increasingly discussed in the literature and among facial plastic surgeons emphasizing the importance of patient selection
- Overaggressive fat removal creating a “gaunt” look.
- Excessive submalar hollowing.
- Accelerated appearance of aging.
- Need for fat grafting or fillers years later.
Technical Pearls to Avoid Errors
- Conservative resection is generally safer than aggressive removal.
- Remove only the amount that passively herniates out of the incision or with gentle dissection and traction
- Compare both sides before completing the procedure.
- Maintain awareness of the parotid duct.
- Consider the patient’s facial aging pattern before surgery.
- When uncertain, under-resection is usually preferable to over-resection.
Aggressive resection in a patient with poor indications (non-round face) is the most common error that can produce a permanent hollow appearance that becomes more noticeable with age.
Dr. Barry Eppley
Plastic Surgeon