

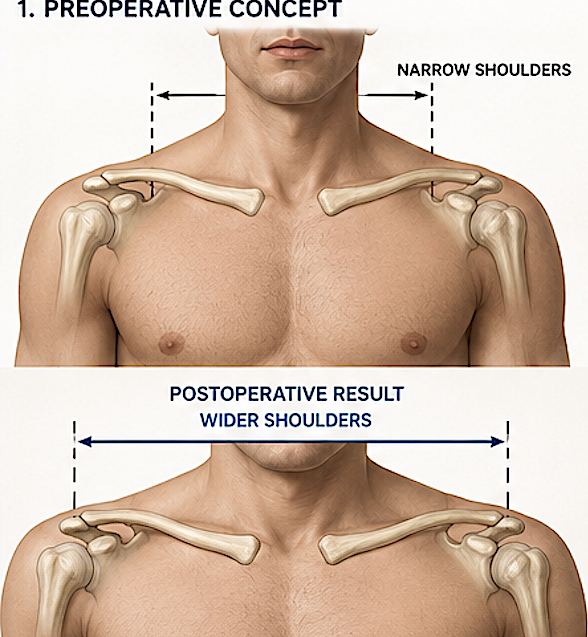
Shoulder widening by clavicle lengthening osteotomies is the opposite of shoulder narrowing surgery. Rather than shortening the clavicles, the bones are divided (osteotomy) and immediately lengthened to increase biacromial shoulder width.
Indications
This is a rare procedure that may be considered for:
- Congenitally narrow shoulders.
- Patients seeking greater upper body width for aesthetic masculinization.
- Selected reconstructive cases following trauma or congenital deformity.
Surgical Concept
The operation involves:

- Making an oblique or sagittal split osteotomy in the midshaft clavicle.
- Creating the maximum amount of clavicle bone lengthening that the soft tissues of the shoulder will permit and securing it with the application of a superior plate and bicortical screws.
- The partial thickness bone defects created by lengthening of the sagittal split osteotomy are filled in with solid corticocancellous cadaveric bone grafts,
- Allowing the bone graft and sagittal split osteotomies to heal over several months.
![]() One potential osteotomy method of clavicle lengthening is a transverse bone with the application of a bone graft in the full thickness interpositonal gap created by the bone lengthening. This approach has several theoretical advantages including a simpler osteotomy cut and the push of the full thickness bone graft on the outer clavicle bone (greater lengthening??). But it would require a longer healing time as bone regeneration must occur across the entire bone graft.length. As a result I have yet to use this clavicle bone lengthening technique.
One potential osteotomy method of clavicle lengthening is a transverse bone with the application of a bone graft in the full thickness interpositonal gap created by the bone lengthening. This approach has several theoretical advantages including a simpler osteotomy cut and the push of the full thickness bone graft on the outer clavicle bone (greater lengthening??). But it would require a longer healing time as bone regeneration must occur across the entire bone graft.length. As a result I have yet to use this clavicle bone lengthening technique.
How Much Widening is Possible?
The clavicle can generally be lengthened by:
- 10–15 mm reliably in a single-stage procedure.
- 15–20 mm in carefully selected patients using structural bone grafts.
- Greater amounts usually require gradual distraction osteogenesis, which is considerably more complex.
Because both clavicles are lengthened, total shoulder width increases by approximately twice the amount of lengthening:
- 10 mm per clavicle ? ~20 mm (2 cm) increase in shoulder width.
- 15 mm per clavicle ? ~30 mm (3 cm) increase.
- 20 mm per clavicle ? ~40 mm (4 cm) increase.
Technical Challenges
Compared with clavicle shortening, lengthening is substantially more difficult because it requires:
- Maintenance of fixation across a gap.
- Bone graft healing.
- Protection of the underlying brachial plexus and subclavian vessels.
- Restoration of clavicular rotation and alignment.
- Fighting against the resistance off the soft tissue attachments of the shoulder girdle
As the lengthening increases, so do the risks of:
- Nonunion.
- Plate failure.
- Bone graft resorption.
- Shoulder stiffness.
Functional Considerations
The clavicle acts as a strut that positions the shoulder away from the chest. Moderate lengthening generally improves shoulder width without significantly altering shoulder mechanics. This is because the attached scapula and humeral soft tissues will not permit ‘excessive lengthening’ to occur that would result in affecting shoulder range of motion.
My Perspective
From a purely biomechanical standpoint, clavicle lengthening is considerably more demanding than clavicle shortening. Decreasing clavicle length is a lot easier than increasing it. While widening of 3 4cm overall is realistically achievable in most patients, larger increases require a gradual distraction method which to date remains elusive in terms of practical device application.
Dr. Barry Eppley
Plastic Surgeon