

 The shape and position of the bony orbit is one of the most important anatomic factors in the development of undereye hollowing and a negative orbital vector. While aging and soft tissue descent contribute to tear troughs, many younger patients have these features because of the underlying skeletal anatomy.
The shape and position of the bony orbit is one of the most important anatomic factors in the development of undereye hollowing and a negative orbital vector. While aging and soft tissue descent contribute to tear troughs, many younger patients have these features because of the underlying skeletal anatomy.
The Normal (Positive Orbital Vector)
In a well-supported midface:
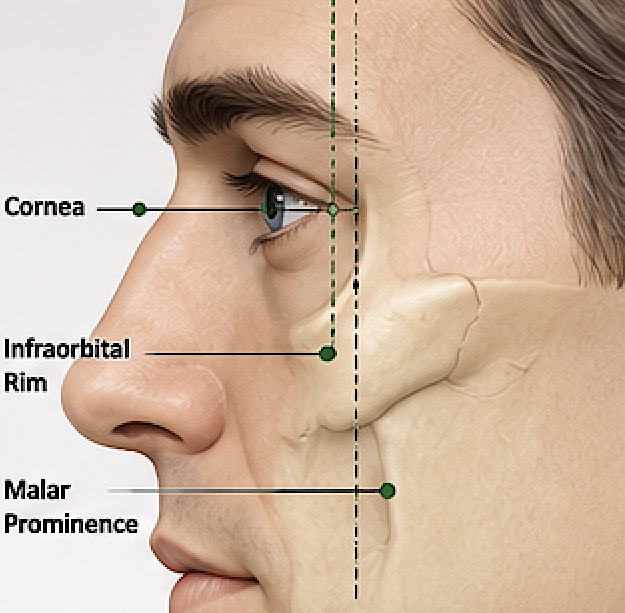

- The infraorbital rim projects forward.
- The upper cheek (malar eminence) sits at or slightly in front of the cornea when viewed from the side.
- The lower eyelid has a gradual transition into the cheek.
- The globe appears well supported by the surrounding bone.
This forward projection minimizes shadows beneath the eyes.
The Negative Orbital Vector
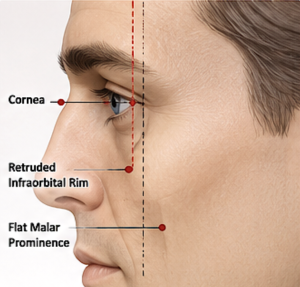

A negative orbital vector occurs when the eyeball projects farther forward than the infraorbital rim and upper cheek soft tissues (not necessarily the bone) on profile view.
This is caused by:
- Posterior positioning (retrusion) of the infraorbital rim
- Underdevelopment of the maxilla beneath the orbit
- Reduced projection of the cheekbone (malar complex)
Rather than being excessively prominent, the eyes often only appear prominent because the surrounding bone is deficient.
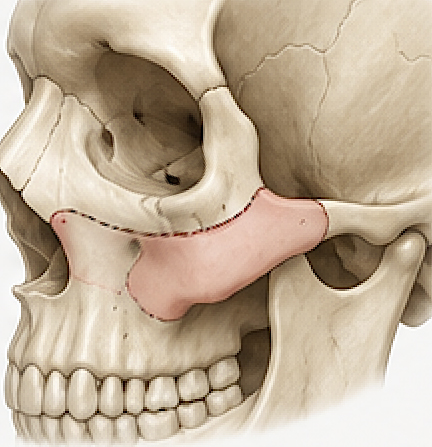
Bony Characteristics
Patients with significant undereye hollowing often have:
- Retruded infraorbital rims
- Shallow anterior projection of the maxilla
- Flat malar prominence
- A steep transition from lower eyelid to cheek
- Reduced skeletal support beneath the orbital fat
- Scleral show
- Pseudo promimemt eyes
This creates a depression beginning immediately below the lower eyelid.
Why Hollowing Occurs
The lower eyelid soft tissues drape over a recessed bony foundation.
As a result:
- Shadows develop beneath the eye.
- The tear trough becomes more visible.
- Orbital fat may appear to bulge despite normal fat volume because the surrounding bone is set farther back.
- Aging exaggerates these findings as skin elasticity decreases.
Clinical Implications
For patients whose primary problem is skeletal deficiency, procedures that tighten skin or remove fat often provide only limited improvement.
Instead, reconstruction of the underlying framework may be indicated, including:
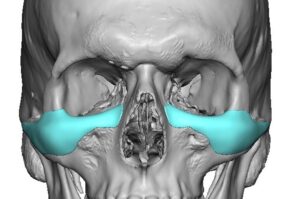
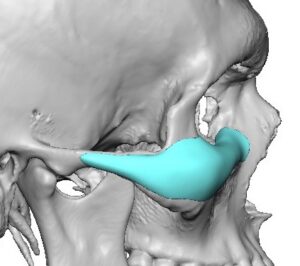
- Custom infraorbital implants
- Infraorbital-malar implants
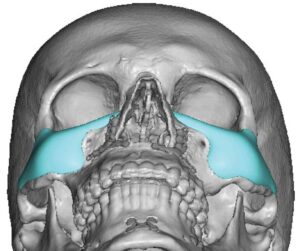
- Infraorbital-maxillary implants for more extensive deficiency
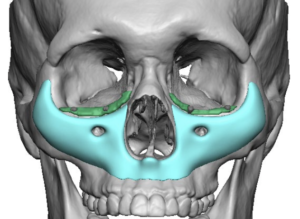
- In severe cases, a custom midface mask implant to restore projection across the orbital rims, cheeks, and upper maxilla
The goal is to move the skeletal foundation forward, reducing the lid-cheek step-off and creating a smoother, more youthful transition from the lower eyelid to the cheek.
Key Concept
Undereye hollowing is often a skeletal problem first and a soft tissue problem second. The greater the retrusion of the infraorbital rim and upper maxilla, the greater the negative orbital vector and the more pronounced the tear trough and lower eyelid hollowing. This is why patients with congenital midface deficiency frequently develop these features at a young age, long before significant facial aging occurs.
Dr Barry Eppley
Plastic Surgeon