


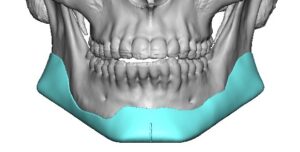
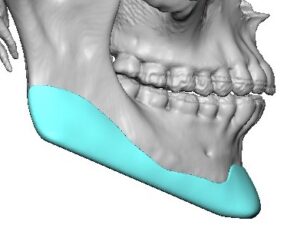
 The submental approach is the most common method for placement of a one-piece custom jawline implant because it provides direct access to the chin and both mandibular body regions through a single, well-hidden incision beneath the chin through which the implant is introduced. It is particularly advantageous for large wraparound implants that extend from angle to angle.
The submental approach is the most common method for placement of a one-piece custom jawline implant because it provides direct access to the chin and both mandibular body regions through a single, well-hidden incision beneath the chin through which the implant is introduced. It is particularly advantageous for large wraparound implants that extend from angle to angle.
However intraoral access is still needed for an adequate subperiosteal dissection over the jaw angles as well as to guide implant placement and screw fixation.
Surgical Technique
Incision(s) and Pocket Dissection
 A 3 to 4 cm incision is placed in the natural submental crease, approximately 1.5 to 2 cm behind the chin point. Dissection proceeds through the subcutaneous tissue to the chin bone. The periosteum is incised, and a subperiosteal pocket is developed over the entire chin and back along the inferolateral border of the mandible on both sides.
A 3 to 4 cm incision is placed in the natural submental crease, approximately 1.5 to 2 cm behind the chin point. Dissection proceeds through the subcutaneous tissue to the chin bone. The periosteum is incised, and a subperiosteal pocket is developed over the entire chin and back along the inferolateral border of the mandible on both sides.
Long periosteal elevators are used to extend the pocket posteriorly along the mandibular body toward each angle while remaining beneath the periosteum. Care is taken to identify and protect the mental nerves as the dissection passes under the mental foramina. But this anterior dissection along is. Not adequate for complete jaw angle (mandibular ramus) pocket development. Two additional intraoral incisions are needed (paired posterior vestibular incisions behind the 2nd molars) for full subperiosteal dissection and ligamentous elevation/release to precisely match the custom implant design.
Implant Placement
 Silicone The sterilized implant is folded or gently flexed as needed and inserted through the submental incision. Because custom silicone implants are flexible, even large implants can usually be delivered through this relatively small incision. The implant is then unfolded and guided into its exact bony position using the patient’s CT-based design as the template. It sounds easy but the jaw angle implant placement is always a challenge given that the working need of the implant is opposite the incisional access.
Silicone The sterilized implant is folded or gently flexed as needed and inserted through the submental incision. Because custom silicone implants are flexible, even large implants can usually be delivered through this relatively small incision. The implant is then unfolded and guided into its exact bony position using the patient’s CT-based design as the template. It sounds easy but the jaw angle implant placement is always a challenge given that the working need of the implant is opposite the incisional access.
PEEK/Medpor/Titanium These very rigid materials require a segmentalize design and placement approach (multiple pieces) The chin segments are passed through the submental incision while the jaw angle sements are passed intraorally through the intraoral posterior vestibular incisions. Alignment/assembly of the multipiece implant design is then done once all pieces are inside the subperiosteal pocket. Contrary to popular perception there is no snap fitting of the implant pieces together. Putting them together as designed is always a challenge with the limited visibility provided by the three small incisions.
Implant Fixation
 Precise positioning is confirmed by palpation of the mandibular borders and symmetry assessment. The implant is then secured with 2 to 4 titanium microscrews, typically placed through the chin and mandibular body portions of the implant. Screw fixation is essential at all three corners (chin and jaw angles) to prevent migration and ensure long-term positional stability. Incisional closure is done with small resorbable sutures.
Precise positioning is confirmed by palpation of the mandibular borders and symmetry assessment. The implant is then secured with 2 to 4 titanium microscrews, typically placed through the chin and mandibular body portions of the implant. Screw fixation is essential at all three corners (chin and jaw angles) to prevent migration and ensure long-term positional stability. Incisional closure is done with small resorbable sutures.
Advantages
- Single hidden incision beneath the chin
- Direct visualization of the chin and mandibular body
- Still requires bilateral intraoral incisions for access to the more posterior jaw angles
- Lower risk of intraoral bacterial contamination than three intraoral incisions
- Secure screw fixation at the three jaw corners
Limitations
An adequately sized posterior subperiosteal pocket over each jaw angle can not be adequately done from the submental incision. Even with long instruments one should not rely on blind dissection for jaw angle pocket creation. A direct intraoral incision over the angles is also needed to supplement the submental one. Only if wrap around jaw implant has a limityed jaw angle component or stops short of it should only a single submental incision be used.

 Overall, the submental approach has become the preferred technique for insertion of most silicone custom wraparound jawline implants, offering excellent implant positioning, stable fixation, and a well-concealed scar while avoiding dragging the implant through the oral cavity. All other implant materials requite segmentalized designs and partial implant introduction through the oral cavity.
Overall, the submental approach has become the preferred technique for insertion of most silicone custom wraparound jawline implants, offering excellent implant positioning, stable fixation, and a well-concealed scar while avoiding dragging the implant through the oral cavity. All other implant materials requite segmentalized designs and partial implant introduction through the oral cavity.
Dr. Barry Eppley
Plastic Surgeon