

 One of the paradoxes of custom facial implants is that while they provide the most precise method of facial skeletal augmentation, they also have a higher revision rate than most standard cosmetic implant procedures and almost any other aesthetic facial surgery. Depending on the facial region and the surgeon’s experience, revision rates of 15–30% are not uncommon. This is not because the implants fail mechanically, but because patients seek perfection rather than improvement.
One of the paradoxes of custom facial implants is that while they provide the most precise method of facial skeletal augmentation, they also have a higher revision rate than most standard cosmetic implant procedures and almost any other aesthetic facial surgery. Depending on the facial region and the surgeon’s experience, revision rates of 15–30% are not uncommon. This is not because the implants fail mechanically, but because patients seek perfection rather than improvement.
The reasons can be divided into several categories.
1. Higher Patient Expectations (The #1 Reason)
Patients choosing custom implants are usually:
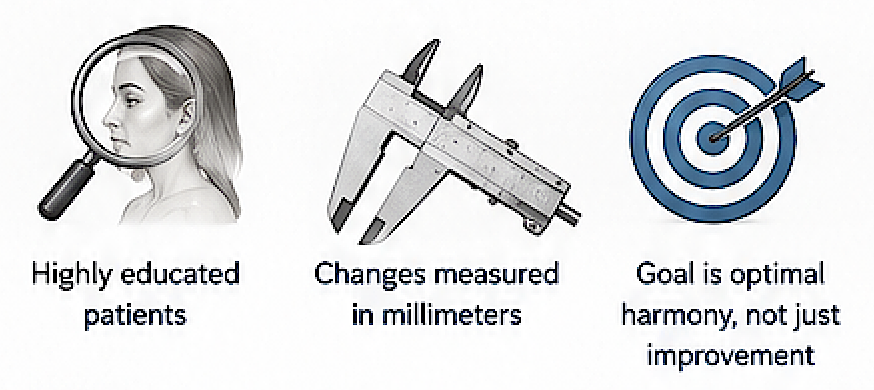
- Highly knowledgeable and have researched extensively.
- Looking for correction of subtle skeletal deficiencies.
- Often dissatisfied with previous surgeries.
- Seeking facial balance measured in millimeters.
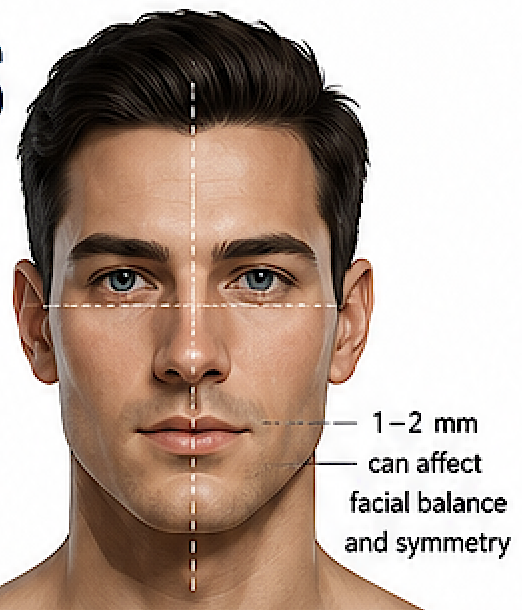
Unlike breast augmentation or chin implants, where patients often desire obvious improvement, custom facial implant patients frequently notice differences of 1–2 mm.
When CAD software allows an implant to be designed to 0.5 mm precision, patients naturally expect the same level of perfection in the final appearance—even though the overlying soft tissues cannot reproduce that level of precision.
2. Facial Symmetry Is Impossible
The human face is inherently asymmetric.
CT-based implant design reveals:
- asymmetric orbits
- different zygomatic positions
- unequal mandibular angles
- variable soft tissue thickness
- muscular asymmetry
A perfectly symmetric implant placed on an asymmetric skeleton will not necessarily produce a symmetric face.
Likewise, making implants asymmetric to compensate for skeletal asymmetry does not always compensate for soft tissue differences.
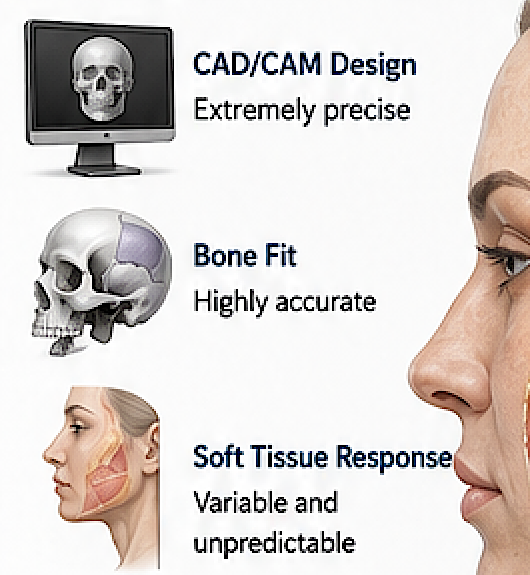
3. Soft Tissue Behavior Is Difficult to Predict
Implants change bone projection.
Patients see skin.
Soft tissues vary tremendously:
- thickness
- elasticity
- fat distribution
- muscle tone
- scar contracture
- age
For example:
A 6 mm cheek implant may create:
- 5 mm visible projection in one patient
- 3 mm in another
- 7 mm in a thin individual
Current software predicts the implant very accurately, but it cannot yet reliably predict the overlying soft-tissue response.
4. Multiple Aesthetic Variables Are Being Changed
Many custom implant patients undergo simultaneous augmentation of:
- forehead
- brow bone
- infraorbital rims
- cheeks
- paranasal area
- jawline
- chin
Each implant may individually be excellent.
The combined aesthetic balance may still need refinement.
It is much like tailoring a custom suit—the first fitting is often excellent, but minor alterations produce the best final result.
5. Computer Precision Exceeds Surgical Precision
Modern CAD design is accurate to fractions of a millimeter.
Surgical placement is affected by:
- tissue resistance
- exposure limitations
- fixation position
- soft tissue compression
- postoperative swelling
Even a perfectly fitting implant may sit 1–2 mm differently than intended.
This difference is often invisible on CT but noticeable in facial aesthetics.
6. Custom Implants Invite Fine-Tuning
Unlike standard implants, custom implants can easily be modified.
Revision implants may involve:
- adding 2 mm
- removing 3 mm
- blending an edge
- extending an implant
- shortening a border
Because redesign is relatively straightforward, surgeons and patients are more willing to pursue incremental refinements.
7. Revision Does Not Usually Mean Failure
Many revisions involve:
- increasing projection
- decreasing projection
- smoothing transitions
- correcting edge visibility
- improving symmetry

These are refinements rather than corrections of complications.
In many series, true complications (infection, exposure, displacement) occur far less frequently than aesthetic refinements.
8. Surgeons Are Still Learning
Custom facial implants remain a niche procedure.
Many surgeons perform only a handful each year.
Success depends on understanding:
- facial aesthetics
- skeletal anatomy
- implant biomechanics
- soft tissue behavior
- CAD design principles
There is a significant learning curve, and experience tends to reduce revision rates.
9. The Procedures Often Address Complex Problems
Many patients are not “primary cosmetic” cases.
Instead they present after:
- V-line surgery
- orthognathic surgery
- implant removal
- trauma
- congenital asymmetry
- prior fat grafting
- previous unsuccessful implants
These challenging starting points increase the likelihood that staged refinement will be needed.
Why Revision Rates Differ by Facial Region
Not all custom facial implants carry the same likelihood of revision:
|
Region |
Typical Revision Risk |
Common Reason |
|
Chin |
Low |
Projection adjustments |
|
Jawline |
high |
Width, angle definition, symmetry |
|
Cheek |
Moderate |
Projection and transition zones |
|
Infraorbital |
Moderate |
Extremely sensitive aesthetics; 1–2 mm differences are noticeable |
|
Forehead |
Low |
Large, smooth contour changes are generally forgiving |
|
Midface mask |
Low |
Multiple aesthetic vectors interacting simultaneously |
The Bottom Line
The relatively high revision rate of custom facial implants is primarily a consequence of the pursuit of aesthetic precision rather than a high complication rate. Modern imaging, CAD design, and manufacturing allow implants to fit the underlying skeleton with remarkable accuracy, but the final appearance is governed by the patient’s soft tissues and highly subjective aesthetic goals. As a result, many revisions are elective refinements—small changes in projection, contour, or symmetry—rather than treatment of implant failure or surgical complications.
In experienced hands, the complication rate (infection, malposition, exposure) is generally low, while the revision rate reflects the desire to optimize an already good result. This distinction is important when counseling patients: a revision after custom facial implant surgery often represents the final stage of achieving an individualized aesthetic outcome, not a failure of the original operation.
Dr. Barry Eppley
Plastic Surgeon