


 A submental soft tissue chin pad excision is a direct surgical procedure designed to reduce the bulk of the soft tissue over the bony chin (chin pad). It is most useful in patients whose chin appears overly full despite having a normal chin bone projection. The excess is usually a combination of fibrofatty tissue, subcutaneous fat, and occasionally a thickened mentalis muscle.
A submental soft tissue chin pad excision is a direct surgical procedure designed to reduce the bulk of the soft tissue over the bony chin (chin pad). It is most useful in patients whose chin appears overly full despite having a normal chin bone projection. The excess is usually a combination of fibrofatty tissue, subcutaneous fat, and occasionally a thickened mentalis muscle.
Liposuction should never be performed in the soft tissue chin pad for reduction due to a high risk of irregularities and ineffectiveness due to its fibrofatty soft tissue composition. Conversely direct excision of the chin pad is far more effective as it permanently reduce both fat and dense fibrous tissue while allowing precise contouring with little risk of irregularities.
Ideal Candidates
This procedure works best for patients with:
- A thick, bulky chin pad that is excessively mobile
- Dynamic chin pad ptosis
- Fatty appearing chin
- A well defined submental skin crease with a convexity anterior to it in profile
It is less effective when fullness is due primarily to:
- An overprotected or long chin bone
- Non-moble chin pad
- Class III malocclusion
Surgical Technique
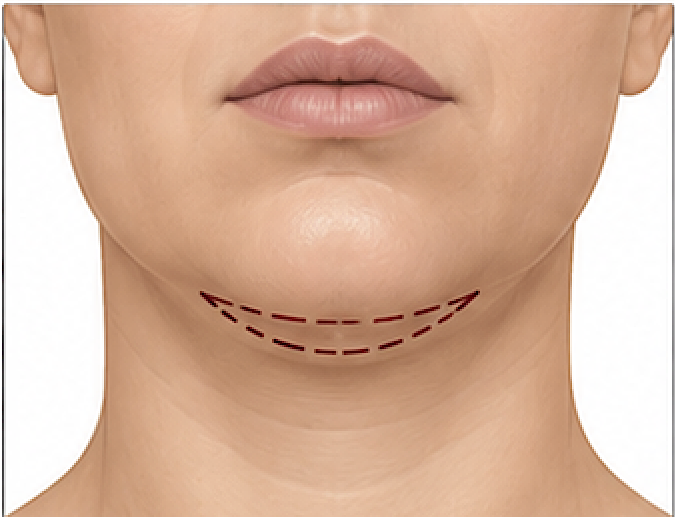
An elliptical full thickness chin pad excision that is either centered over or anterior to an existing submental skin crease.
Excision Design

The excision should be elliptical and a good design rule is:
- Length : Height = approximately 3–4 : 1
For example:
- 6 cm long ? 1.5–2 cm high
- 5 cm long ? 1.3–1.7 cm high
This ratio minimizes dog-ear formation and distributes tension evenly,
Tissue Excision Amount
- Small chin pad reduction: 5–7 mm
- Moderate chin pad reduction: 7–10 mm
- Large chin pad reduction: 10–15 mm
The goal is reduce as much chin pad as possible while keeping the scar line under the point of maximum chin projection and preventing a long scar line that is visible in profile.
Potential Risks
- Temporary numbness beneath the chin
- Minor contour irregularities
- Hematoma or seroma
- Scar widening (usually well hidden in the submental crease)
- Under- or over-resection
Technical Pearls
- A wide full-thickness excision of the excess soft tissue chin pad anterior to the submental crease is the key to an effective reduction.
- Taper the excision gradually at both ends of the ellipse.
- Avoid abrupt thickness transitions to prevent palpable ridges.
A direct submental soft tissue chin pad excision is a valuable but relatively uncommon procedure. In appropriately selected patients—particularly those with a dense, fibrofatty submental pad—it can reduce the size of the chin and eliminate dynamic chin pad ptosis.
Case Study

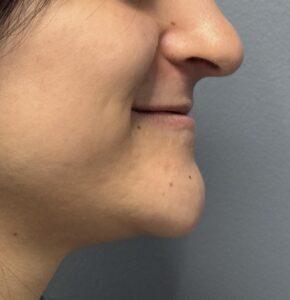 This young female had a congenital large soft tissue chin pad that had a pronounced dynamic chin pad ptosis. While she had adequate chin bone projection it was not excessive. The chin pad was quite mobile from the end of the chin bone with a fleshy consistency,
This young female had a congenital large soft tissue chin pad that had a pronounced dynamic chin pad ptosis. While she had adequate chin bone projection it was not excessive. The chin pad was quite mobile from the end of the chin bone with a fleshy consistency,
 Preoperatively an excision pattern was marked using the submental skin crease as the posterior incision line. Centrally it measured 17 mm with a 50 mm length.
Preoperatively an excision pattern was marked using the submental skin crease as the posterior incision line. Centrally it measured 17 mm with a 50 mm length.



 Under an anesthesia, a full thickness, chin pad excision utilizing the marks was performed. No underlying chin bone was removed. The soft tissue chin pad was mobilized off of the bone super purely and then brought over it to close in multiple layers, but they scar line under the point of maximal, chin projection.
Under an anesthesia, a full thickness, chin pad excision utilizing the marks was performed. No underlying chin bone was removed. The soft tissue chin pad was mobilized off of the bone super purely and then brought over it to close in multiple layers, but they scar line under the point of maximal, chin projection.

 The improvement in the size of the chin pad could be immediately appreciated. It would be fully expected that the dynamic chin pan ptosis will now be fully resolved. The only long-term question is how well does the scar do and will eventually require scar revision?
The improvement in the size of the chin pad could be immediately appreciated. It would be fully expected that the dynamic chin pan ptosis will now be fully resolved. The only long-term question is how well does the scar do and will eventually require scar revision?
Discussion
In a horizontal elliptical excisions of the chin pad what is the height to length ratio to avoid tissue bunching at each end?
For a horizontal fusiform (elliptical) excision, the classic surgical principle to minimize dog-ears (tissue bunching) at the ends is:
- Length : Width = 3:1 at a minimum
- 4:1 is often preferred in areas with thick skin or limited tissue mobility
- 5:1 may be necessary in very dense tissues
Height-to-length ratio:
|
Ellipse Height (maximum width) |
Ellipse Length |
Height:Length Ratio |
|
1 cm |
3 cm |
1:3 (0.33) minimum |
|
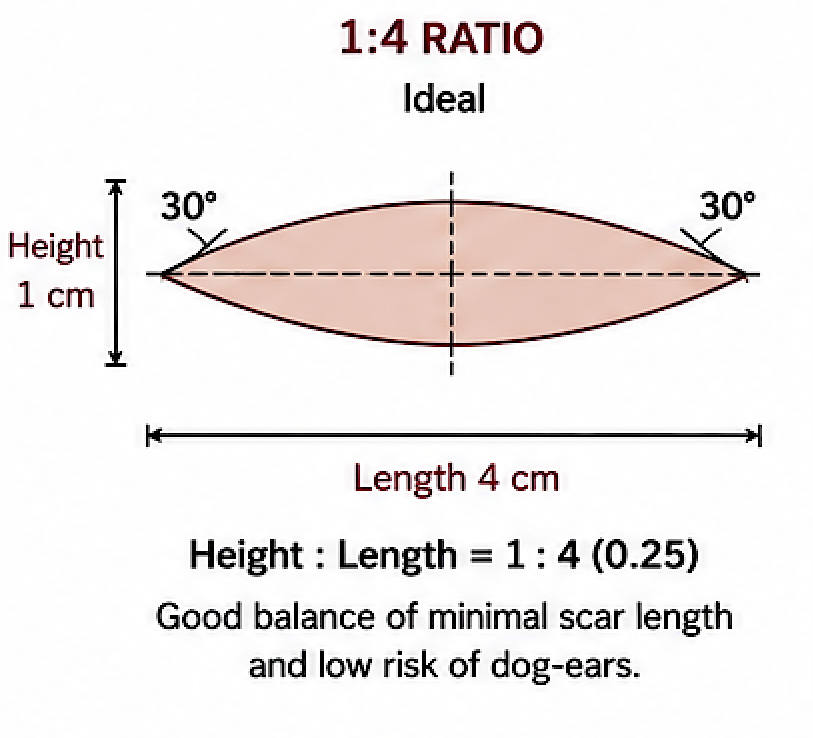
1 cm |
4 cm |
1:4 (0.25) ideal for many facial/body closures |
|
1 cm |
5 cm |
1:5 (0.20) for high-tension areas |
Tip Angle
Another equally important variable is the apical angle.
- 30° is considered ideal.
- Less than 30° creates unnecessarily long scars.
- Greater than 45° markedly increases the risk of standing cone deformities (dog-ears).
Practical Plastic Surgery Guidelines
For most facial horizontal excisions:
- Height:Length = 1:3.5–1:4
- 30° apical tips
- Undermine at least one ellipse width on each side when appropriate.
- Close the deep dermis first to distribute tension.
If Dog-Ears Still Occur
Dog-ears are influenced by more than ellipse geometry:
- unequal skin thickness
- asymmetric undermining
- unequal wound edge lengths
- closure under tension
- wound orientation relative to relaxed skin tension lines
In these cases, extending the excision another 10–20% of its length or excising a small Burow’s triangle is often preferable to excessive tension.
For submental chin pad excisions design ellipses closer to 4:1 is the least likely to create residual end bunching (dog ears). But this may not always be prsctical of that makes the scar length too long
Key Points
1) Submental chin pad excisions where a defined submental skin crease exists uses a wedge excision anterior to the crease.
2) The wedge excision height to with ratio is three or four to one, depending upon how long a scar length it creates.
3) The amount of soft tissue excision that is done is mindful of the scar length, keeping it less than a vertical line dropped down from the corners of the mouth.
Barry Eppley, MD, DMD
World-Renowned Plastic Surgeon