

A transpalpebral Endotine brow lift is a less commonly performed variation of brow elevation in which the brow is lifted through an upper eyelid (blepharoplasty) incision rather than through scalp incisions. The Endotine device is used to secure the elevated brow tissues to the frontal bone. This technique combines an upper blepharoplasty with a direct internal brow lift and fixation.
Advantages
- No scalp incisions
- Easily combined with upper blepharoplasty
- Avoids scalp numbness and visible scalp scars
- Direct access to the brow retaining ligaments
- Excellent visualization of the lateral brow
- Less postoperative forehead discomfort than some endoscopic approaches
Limitations
This approach is not a substitute for a full endoscopic brow lift.
Compared with an endoscopic brow lift:
- Less superior forehead dissection can limit the amount of brow elevation.
- Central forehead elevation is generally less effective.
- Brow elevation is typically more modest (often around 3–6 mm).
- Best suited for correcting lateral brow ptosis rather than significant medial brow descent.
Ideal Candidates
The transpalpebral Endotine brow lift is particularly useful for patients who have:
- Mild to moderate lateral brow descent
- Hooding of the upper eyelids due in part to brow ptosis
- A desire to combine brow elevation with upper blepharoplasty
- Minimal forehead wrinkles requiring treatment
It is less suitable for patients with:
- Marked brow ptosis
- Heavy foreheads
- Significant forehead skin excess
- A need for substantial medial brow elevation
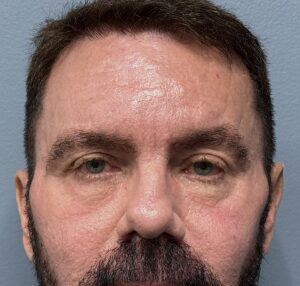
Case Study
This male was bothered by his heavy brows, particularly at the outer corners and excessiv upper eyelid skin. He desired removal of upper eyelid skin with some elevation of the tail of the eyebrow. He had no concerns about the medial or inner half of this eyebrows.
The surgical technique consisted of:
Upper eyelid incision
- A standard upper blepharoplasty incision is made within the upper eyelid crease.
- Excess skin and limited fat removal..
Suborbicularis dissection
- Dissection proceeded superiorly beneath the orbicularis oculi muscle to the superior orbital rim.
- The periosteum was incised approximately 5mm above the rim.
Forehead release
- Subperiosteal dissection extended upward over the frontal bone.
- The lateral orbital thickening and brow retaining ligaments were released to mobilize the brows..
Endotine placement


- A small hole was drilled into the frontal bone several centimeters above the orbital rim.
- The Endotine implant is secured to the bone.
- The elevated forehead tissues are lifted ands engaged onto the implant’s multiple tines, maintaining the brow in its new position.
Closure
- The eyelid incision is closed small fast resorbing sutures
- No scalp incisions are required.
Results
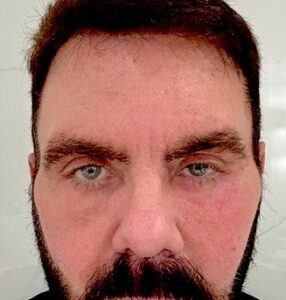
His 6 week results showed good improvement with no viisble scarring.
Discussion
The transpalpebral Endotine brow lift enjoyed its greatest popularity in the early to mid-2000s, particularly among surgeons performing cosmetic eyelid surgery. While the concept of internal brow fixation remains sound, the use of the Endotine implant has declined as many surgeons now achieve similar results with absorbable sutures, drill-hole fixation, or suture anchors through the same transpalpebral approach. The operation itself remains a valuable option for selected patients, especially when the primary goal is lateral brow elevation performed concurrently with upper blepharoplasty.
For many patients undergoing cosmetic upper eyelid surgery today, a transpalpebral brow lift—whether using Endotine fixation or modern suture-based techniques—can provide a more harmonious rejuvenation by addressing both eyelid skin excess and the brow position that contributes to upper eyelid hooding.
Dr. Barry Eppley
Plastic Surgeon