


The size and shape of the clavicle are among the primary anatomical factors that determine how much shortening can be performed safely.
Several aspects of clavicular anatomy matter:
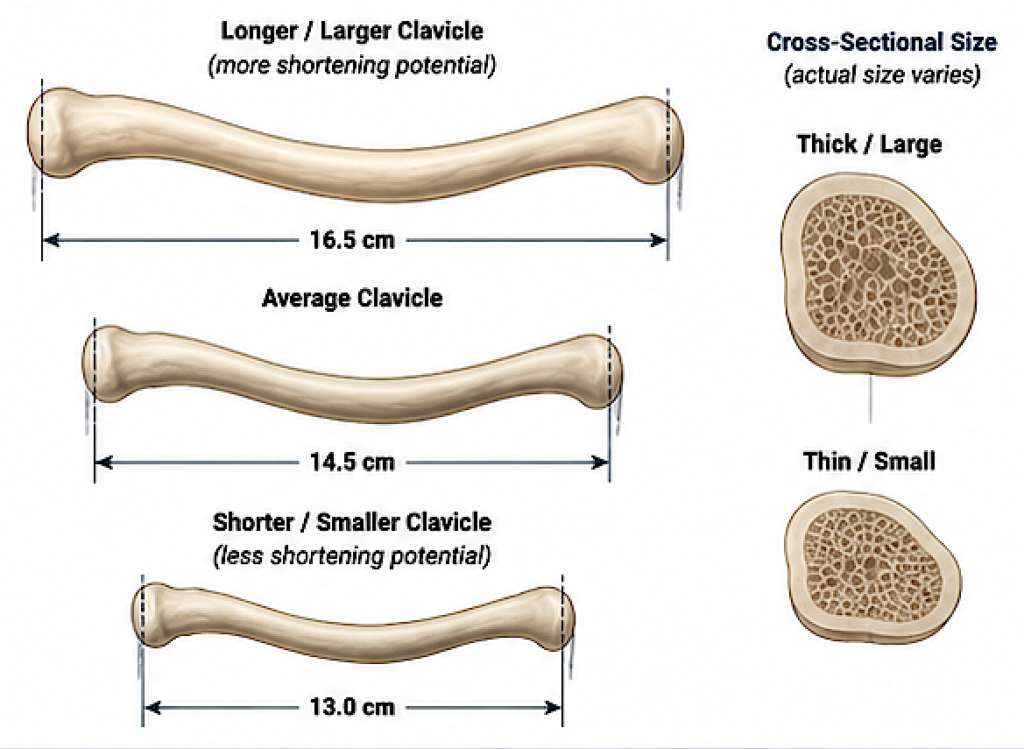
- Overall clavicle length
- A long clavicle provides more “reserve” for shortening.
- A short clavicle reaches biomechanical limits sooner.
- Men generally have clavicles about 15–17 cm long, while women average 13–15 cm, although there is substantial individual variation.
- Cross-sectional size
-
- A thicker clavicle has greater structural strength after fixation.
- A thinner clavicle offers less bone for plate and screw fixation, making very large resections less desirable.
- Curvature (S-shape)
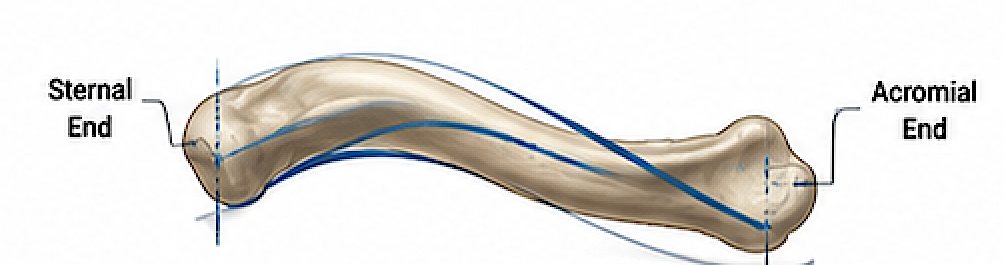
-
- The clavicle is not straight. Its changing curvature influences where the osteotomy can be performed and how well the remaining bone ends match after shortening.
- Excessive shortening can create rotational mismatch if performed at a single osteotomy site.
- Medullary canal size
-
- Larger clavicles typically have a wider intramedullary canal and more cortical bone, providing better fixation characteristics.
Practical limits
From a cosmetic shoulder narrowing standpoint, the limiting factor is usually shoulder biomechanics, not simply bone length.
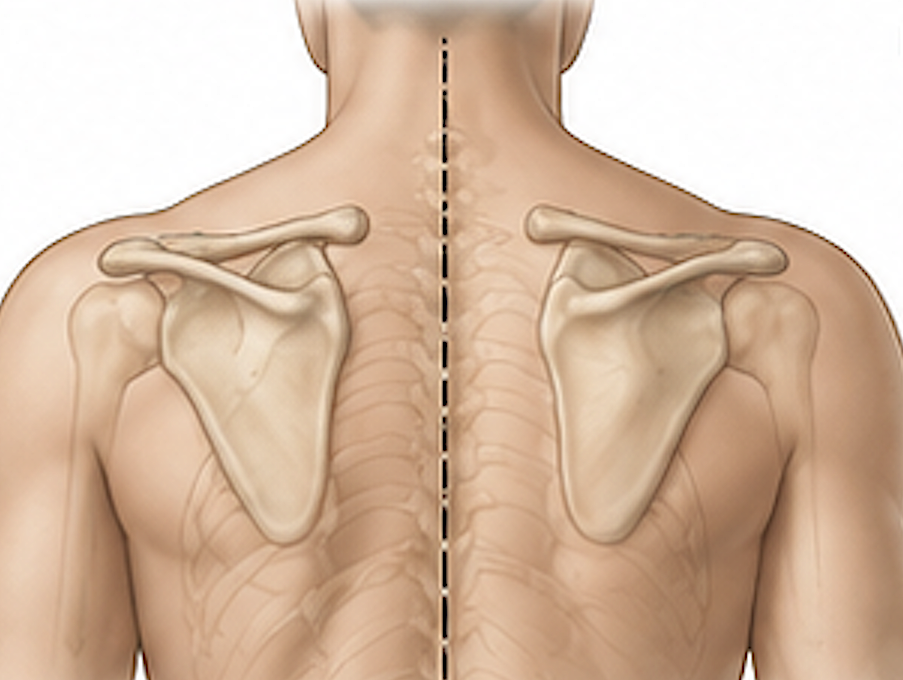
As shortening increases:
- the scapula rotates anteriorly and medially,
- muscle resting lengths change,
- stresses across the acromioclavicular (AC) and sternoclavicular (SC) joints increase.
Even if a clavicle is long enough to remove 30 mm of bone, that does not necessarily mean it should be shortened that much.
Typical relationship
A rough guide is:
|
Clavicle size |
Potential shortening |
|
Small/thin clavicle |
Usually 15–20 mm |
|
Average clavicle |
Usually 20–25 mm |
|
Large/long clavicle |
May tolerate 25–30 mm in carefully selected patients |
These are general estimates rather than fixed limits. The appropriate amount depends on fixation, surrounding anatomy, and the desired shoulder width reduction.
Preoperative planning
A 3D CT scan is the best way to determine an individual’s safe shortening because it allows measurement of:
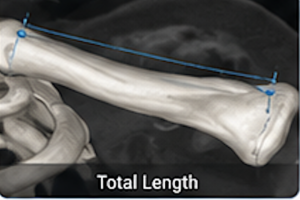
- total clavicle length,
- cortical thickness,
- diameter,
- curvature,
- symmetry,
- predicted postoperative shoulder width.
Rather than asking “How much bone can be removed?”, the more useful question is “How much shoulder narrowing can be achieved while maintaining normal shoulder mechanics?”
In my experience with cosmetic clavicle reduction osteotomies, clavicle size influences the maximum feasible shortening, but the patient’s scapulothoracic mechanics and fixation stability are ultimately the factors that determine the safe upper limit, not the bone length alone.
Dr. Barry Eppley
Plastic Surgeon