

An extended corner of the mouth lift (ECML) is a modification of the traditional corner of the mouth lift (CML) that extends the excision beyond the commissure and onto the lateral upper lip. It is designed for patients in whom simply elevating the oral commissure is insufficient to create a more youthful or aesthetically pleasing smile.
What an Extended Corner of the Mouth Lift Treats
The procedure is useful for patients with:
- Downturned mouth corners
- A long, flat lateral upper lip
- Loss of lateral upper lip vermilion show
- Mild lateral perioral skin laxity
- Residual mouth corner drooping after a facelift
- Congenitally sad or stern resting facial expression
Unlike a standard corner lift, the extended version improves both the position of the commissure and the contour of the lateral upper lip.
Surgical Design

The incision begins at the oral commissure but extends laterally along the vermilion-cutaneous border of the upper lip.
This allows:

- Greater elevation of the commissure
- Shortening of the lateral upper lip
- Increased lateral vermilion show
- Better smoothing of the upper lateral marionette region
- More harmonious transition between the upper lip and mouth corner
The skin excision is typically a carefully designed curved or elliptical wedge that follows natural aesthetic subunits to help camouflage the scar.
Advantages Over a Standard Corner Lift
|
Standard Corner Lift |
Extended Corner Lift |
|
Raises commissure only |
Raises commissure and reshapes lateral upper lip |
|
Limited effect in severe downturn |
Greater correction |
|
Small scar |
Slightly longer scar |
|
Best for isolated mouth corner droop |
Best for combined corner droop and lateral lip aging |
|
Less ability to increase upper lip show |
Increases lateral vermilion exposure |
Ideal Candidates
Patients who typically benefit include:
- Adults over 40 with age-related mouth corner descent
- Younger patients with congenitally downturned commissures
- Patients with naturally long upper lips laterally
- Patients undergoing facial rejuvenation who want a more cheerful resting expression
- Patients combining the procedure with lip advancement
Procedures Commonly Combined
An extended corner lift is frequently combined with:
- Direct lip advancement
- Bullhorn lip lift
- Lower facelift
- Neck lift
- Perioral laser resurfacing
- Chin implant or custom jawline implant
- Buccal fat reduction (selected patients)
The combination with direct lip advancement is particularly effective because the lip advancement improves central vermilion exposure while the extended corner lift improves the lateral lip and commissure, creating a more balanced result.
Limitations
The procedure will not:
- Correct severe marionette folds (fat grafting or facelift may still be needed)
- Lift sagging cheeks
- Replace a facelift
- Improve significant lower facial volume loss
Recovery
Typical recovery includes:
- Mild swelling for 1–2 weeks
- Sutures removed in approximately 5–7 days
- Most bruising resolves within 10–14 days
- Scar maturation continues for 6–12 months
Patients can usually return to normal social activities within 7–10 days, although the incision remains pink for several weeks.
Scarring
The primary tradeoff is a longer scar than with a conventional corner lift. However, when meticulously placed along the vermilion-cutaneous junction and extending within natural facial aesthetic units, the scar generally becomes much less noticeable over time.
Why the Extended Technique Can Produce Better Results
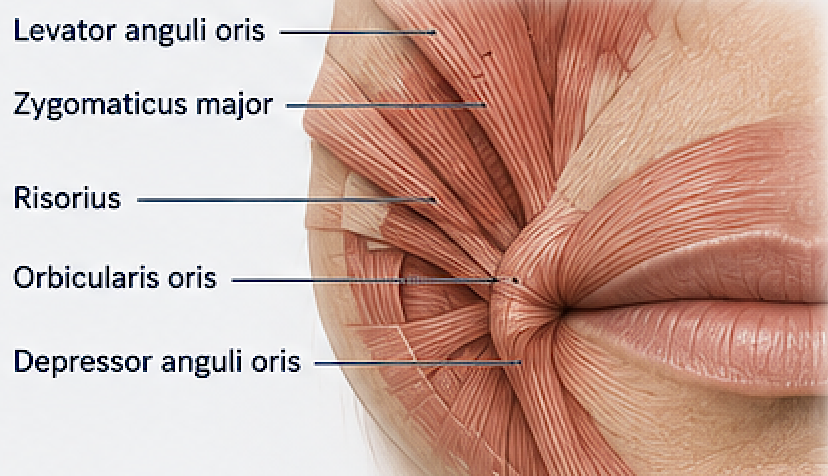 The oral commissure is supported by a complex network of muscles—including the orbicularis oris, depressor anguli oris, levator anguli oris, zygomaticus major, and risorius. Simply lifting the commissure often leaves the adjacent lateral upper lip unchanged, limiting the overall aesthetic improvement. By extending the excision laterally, the surgeon can reposition a larger perioral skin segment, resulting in:
The oral commissure is supported by a complex network of muscles—including the orbicularis oris, depressor anguli oris, levator anguli oris, zygomaticus major, and risorius. Simply lifting the commissure often leaves the adjacent lateral upper lip unchanged, limiting the overall aesthetic improvement. By extending the excision laterally, the surgeon can reposition a larger perioral skin segment, resulting in:
- A smoother lateral lip contour
- Better upper lip eversion laterally
- A more naturally upturned resting expression
- A more balanced smile without an over-pulled appearance
For appropriately selected patients, the extended corner of the mouth lift can provide a more comprehensive and durable improvement than a standard corner lift while preserving a natural appearance.
Case Example

 This young male wanted his sagging mouth corners improved, and this was to be performed at the same time as other facial reshaping procedures. An extended corner of the mouth lift was designed along the lateral upper lip vermilion with an extended isosceles triangle type design. The marked skin was excised in a back cut performed down unto the lower lip to permit the corner to be elevated. The extent of the upper lip lateral vermilion incision is what controls reshaping the entire lateral upper lip vermilion.
This young male wanted his sagging mouth corners improved, and this was to be performed at the same time as other facial reshaping procedures. An extended corner of the mouth lift was designed along the lateral upper lip vermilion with an extended isosceles triangle type design. The marked skin was excised in a back cut performed down unto the lower lip to permit the corner to be elevated. The extent of the upper lip lateral vermilion incision is what controls reshaping the entire lateral upper lip vermilion.

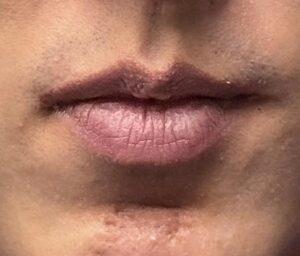

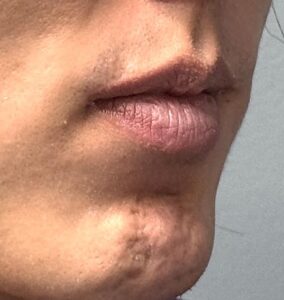
His long-term results showed an improved lateral upper lip shape with an elevated corner and a very acceptable inconspicuous scars.
Discussion
Despite its ability to improve a chronically downturned mouth, corner of the mouth lift (CML) surgery remains a relatively uncommon aesthetic procedure. The reasons are primarily related to patient acceptance, surgeon preference, and the balance between benefit and visible scarring rather than the effectiveness of the operation itself.
1. The Scar Is the Biggest Limiting Factor
The procedure places an incision directly at the oral commissure and often extends onto the upper lip.
While experienced surgeons can camouflage the scar well along the vermilion-cutaneous junction and natural skin creases, it is still a visible facial scar during healing and, in some patients, remains detectable.
Many patients who desire a happier resting expression are reluctant to accept even a small permanent scar.
This is probably the single greatest reason the operation is not performed more frequently.
2. Many Surgeons Are Uncomfortable Trading a Scar for an Aesthetic Improvement
Plastic surgeons are generally trained to minimize facial scars whenever possible.
Since many facial rejuvenation procedures rely on hidden incisions (inside the mouth, hairline, eyelids, or ears), a procedure that intentionally places an incision on the visible face is outside many surgeons’ comfort zone.
As a result, surgeons often recommend alternatives such as:
- Fillers
- Fat grafting
- Neuromodulators
- Facelift surgery
- Laser resurfacing
These treatments may improve the surrounding tissues but often do not directly elevate the oral commissure.
3. The Procedure Is Technically More Demanding Than It Appears
Although the skin excision is small, the operation requires meticulous planning.
Small differences in:
- angle
- rotation
- skin tension
- vermilion alignment
- symmetry
can produce noticeable asymmetries.
Even a 1–2 mm difference between sides may be visible.
Overcorrection produces an unnatural “Joker” appearance, while undercorrection yields little improvement.
4. Patient Selection Is Critical
Not every downturned mouth is caused by skin excess.
The appearance may instead result from:
- heavy marionette folds
- cheek descent
- platysmal laxity
- skeletal deficiency
- lower facial volume loss
- habitual muscle activity
In these patients, a corner lift alone may provide only modest improvement.
The best candidates are those with true commissure ptosis and adequate skin quality, with or without a long lateral upper lip.
5. There Is Limited Formal Training
Most plastic surgery residency programs devote little time to corner of the mouth lifts.
The procedure is learned primarily through:
- individual experience
- facial aesthetic fellowships
- international literature
- self-developed techniques
Consequently, relatively few surgeons become comfortable offering it routinely.
6. Demand Is Lower Than for Other Facial Procedures
Patients commonly seek:
- facelifts
- eyelid surgery
- rhinoplasty
- lip lifts
- neck lifts
Far fewer patients recognize that the corners of the mouth contribute significantly to facial expression.
Many simply describe looking “sad” or “angry” without realizing the oral commissures are a major contributor.
7. Alternatives Are Easier to Offer
Injectable treatments require:
- no incisions
- minimal downtime
- little recovery
- lower upfront cost
Although fillers and Botox generally cannot permanently reposition the commissure, they are often chosen because they avoid surgery.
8. Concerns About Distortion
Surgeons worry about:
- widening the mouth
- altering smile dynamics
- asymmetry
- distortion of the vermilion border
- contracture during healing
When performed properly, these problems are uncommon, but they contribute to hesitation among surgeons who perform the operation infrequently.
Why Interest Is Increasing
Awareness of the procedure has grown with the popularity of facial aesthetic analysis and social media. More patients now recognize that the resting position of the oral commissures has a significant influence on perceived emotion. At the same time, refinements such as the extended corner of the mouth lift, which also shortens the lateral upper lip and increases lateral vermilion show, have expanded the indications and can produce more balanced, natural-looking results in carefully selected patients.
Bottom Line
The corner of the mouth lift is not uncommon because it is ineffective—it is uncommon because it requires accepting a visible facial scar in exchange for a relatively subtle but meaningful aesthetic improvement. For the right patient, however, it remains the only procedure that directly and permanently elevates the oral commissure, something fillers, neuromodulators, lasers, and even facelifts typically cannot achieve predictably on their own. When performed with careful design and meticulous scar placement, it can create a more relaxed, approachable, and youthful resting facial expression with durable results.
Dr. Barry Eppley
Plastic Surgeon