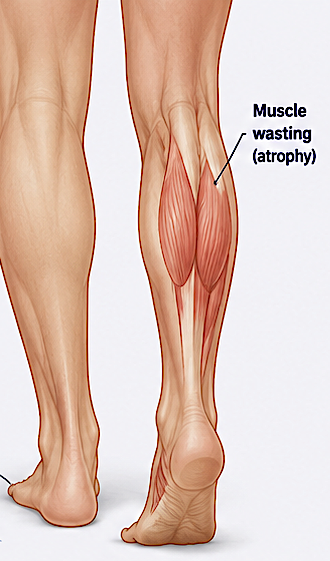


 Calf implants can be a useful reconstructive option in selected patients with Charcot–Marie–Tooth (CMT) disease, particularly when there is severe lower leg muscle wasting (“stork legs”) that causes cosmetic deformity and sometimes difficulty fitting clothing or feeling comfortable socially.
Calf implants can be a useful reconstructive option in selected patients with Charcot–Marie–Tooth (CMT) disease, particularly when there is severe lower leg muscle wasting (“stork legs”) that causes cosmetic deformity and sometimes difficulty fitting clothing or feeling comfortable socially.
A few important considerations make CMT patients different from standard cosmetic calf augmentation patients:
Why calf wasting occurs in CMT
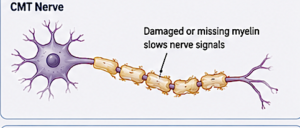
CMT is a hereditary peripheral neuropathy that progressively weakens the distal leg muscles, especially:
- gastrocnemius
- soleus
- peroneal muscle groups
The muscle atrophy is neurologic in origin, so exercise usually cannot restore significant bulk.
Role of calf implants
Silicone calf implants can:
- partially restore lower leg contour
- improve symmetry
- improve psychological confidence/body image
- camouflage severe muscle atrophy
However, implants do not improve muscle strength or neurologic function.
Surgical challenges in CMT patients
Patients with CMT require careful evaluation because they often have:
- very thin soft tissue coverage
- muscle imbalance
- foot deformities (cavus foot, hammertoes)
- gait abnormalities
- sensory changes
- poorer wound healing potential in severe neuropathy
These factors increase risks such as:
- implant visibility/palpability
- malposition
- wound healing problems
- infection
- chronic pain
- asymmetry
Implant placement considerations
In CMT patients:
- subfascial placement is usually preferred but often not possible due to the tight fascia
- Deep subcutaneous or on top of fascia offers a more visible result with less risk
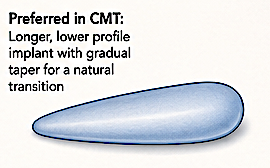
- implant size selection must be conservative
- custom or asymmetric implants may sometimes be beneficial
- bilateral implants are common
Almost always only the medial calf is augmented because the tight tissue will only permit one implant per leg.
Alternative or adjunctive options
Depending on anatomy:
- fat grafting may help mild deformities
- custom implants can help severe asymmetry
- orthopaedic correction of foot deformities may be more functionally important first
Who is a good candidate
Best candidates usually:
- have stable neurologic disease
- realistic expectations
- adequate soft tissue coverage
- no major vascular compromise
- no active ulceration or severe sensory loss
Outcomes
Most published experience is limited to small case series, but cosmetic improvement and patient satisfaction are generally high when patient selection is appropriate.
Dr. Barry Eppley
Plastic Surgeon