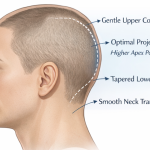
What is Aesthetic Skull Reshaping Surgery
Every day I get inquiries from patients requesting ‘skull reshaping surgery’ without any further specifications or details of their head shape concerns, not recognizing the scope of the general term. A detailed description of what encompasses skull reshaping surgery is described. What is Aesthetic Skull Reshaping Surgery Aesthetic skull reshaping surgery—often called cranial contouring Read More…