Custom Brow Bone Feminization Reversal -Case Study
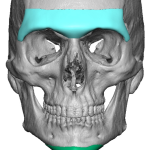
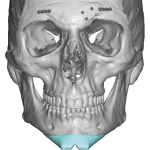
Introduction A custom brow bone implant is a patient-specific facial implant designed to enhance or reconstruct the supraorbital rims (brow ridges). Aesthetically, it is most commonly used for facial masculinization or for correction of flat or recessed brows. With the growing popularity of facial feminization surgery (FFS), custom brow bone implants have also become an Read More…