Challenges in Medpor Facial Implant Removals

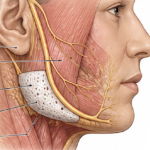
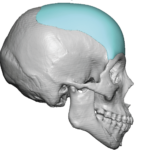
Medpor (porous polyethylene) facial implants are designed to integrate with surrounding tissue, which is great for stability—but that same feature makes removal significantly more difficult than with smooth implants (like silicone). Here are the main challenges surgeons face: 1. Tissue Ingrowth (Primary Issue) Medpor is porous, allowing fibrovascular tissue to grow into it. Over time, Read More…