Decision Tree for Implant vs Genioplasty in Revisions
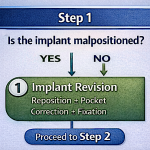
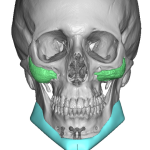
In treating chin implant asymmetries the decision is between implant revision vs. sliding genioplasty. This is how to think about that choice in a structured manner.s Decision Tree: Implant vs. Sliding Genioplasty (Revision Cases) Step 1: Is the implant malpositioned? YES Proceed with implant revision (reposition ± pocket correction ± fixation) NO go to Step Read More…