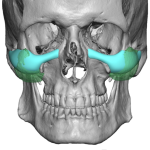
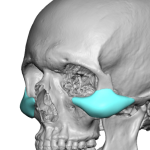
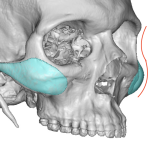
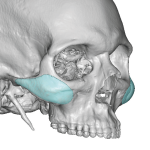
Custom Midface Implants vs Standard Cheek Implants – Comparison Case Study

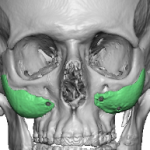
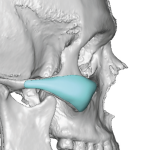
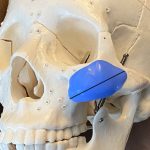
Cheek implants are a well known permanent facial augmentation method that was originally developed for true skeletal deficiencies. Such congenital or developmental deficiencies include: Flat or under-projected cheekbones Poor midface projection despite normal weight Long faces Class II skeletal patterns Patients with weak zygomatic prominence Sunken mid faces Cheek volume loss Cheekbone asymmetries Implants restore Read More…