Brow Bone Reduction: Shaving vs Bone Flap Setback Techiques
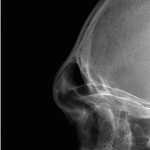
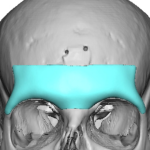
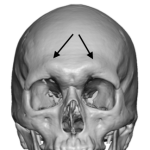
For reducing the over projected brow the question is which bone reduction technique, shaving or osteotomy setback, is needed. Both reduce the bony projection but they do it differently and with different effects. Here is a clear surgical comparison of brow bone shaving vs. frontal sinus setback. Feature Brow Bone Shaving (Burring) Frontal Sinus Setback Read More…