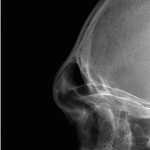
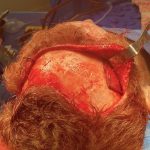
Female Forehead Augmentation – Extended Implant Design in the Backward Sloped Forehead
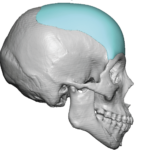
Female forehead augmentation is a cosmetic procedure designed to add volume and create a smoother, more rounded, feminine forehead shape—as opposed to reducing bone (which is done in forehead feminization surgery). What it is A procedure to enhance a flat, concave, or under-projected forehead Aims for a gentle convex contour with a more vertical slope, Read More…