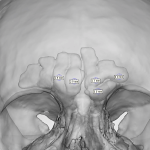
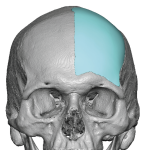
Female Forehead Osteoma Removal Case Example

Forehead osteomas are benign (non-cancerous) bone tumors that commonly appear on the frontal bone of the skull—basically the forehead area. What they are Made of dense, mature bone Typically slow-growing Feel like a hard, immovable lump under the skin Usually painless Why they occur The exact cause isn’t always clear, but possible factors include: Genetics Read More…