

Macrotia Reduction with Middle Third Excision Technique Case Study
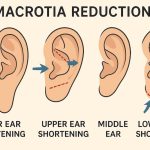
Introduction Vertical ear reduction—also known as vertical ear shortening or macrotia reduction—is a surgical procedure that decreases the overall height of the external ear while preserving its natural contour. It is performed when a patient has macrotia, a condition in which the ears are normally shaped but disproportionately tall. This procedure addresses ear height only Read More…





