Cheekbone Reduction Case Study

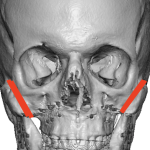
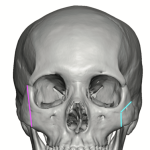
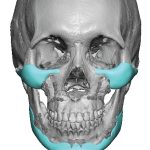
Background Patients seeking facial width reduction are usually focused on the cheeks, which are typically the widest part of the face. This width is primarily due to the zygomatic arch, which must curve outward to allow the temporal muscle to pass beneath it and attach to the ramus of the lower jaw. To narrow facial Read More…