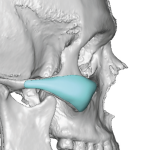
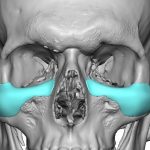
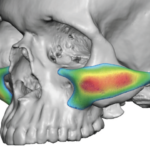
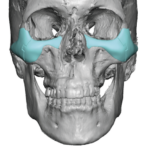
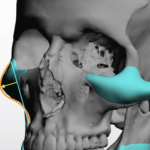
Male vs Female Cheek Implant Augmentation – Aesthetic Shape Differences
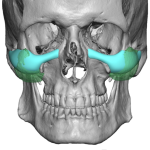
While a variety of off-the-shelf cheek implants are available, none of them provide any guidance about gender specificity. This is unfortunate, as like all facial augmentations, few are non-gender specific or non-binary in nature. Yet this is how most surgeons approach cheek augmentation… locked into choosing whatever is in the catalog believing or hoping that Read More…