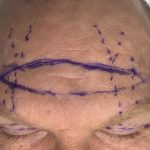
Direct Browlift in Vertical Orbital Dystopia Case Example

A direct browlift is a brow-lifting operation in which skin is removed just above the eyebrow, and the brow is elevated by closing that excision. It is mainly used to treat brow ptosis, especially when the droop affects the upper visual field or creates significant asymmetry. Compared with endoscopic or coronal brow lifts, the direct Read More…